

Prevalence of cartilaginous tumours as an incidental finding on MRI of the knee
- PMID: 25994192
- PMCID: PMC4636526
- DOI: 10.1007/s00330-015-3764-6
Prevalence of cartilaginous tumours as an incidental finding on MRI of the knee
Abstract
Objectives: The purpose was to determine prevalence of enchondromas and atypical cartilaginous tumour/chondrosarcoma grade 1 (ACT/CS1) of the knee on MRI in a large cohort study, namely the Netherlands Epidemiology of Obesity (NEO) study.
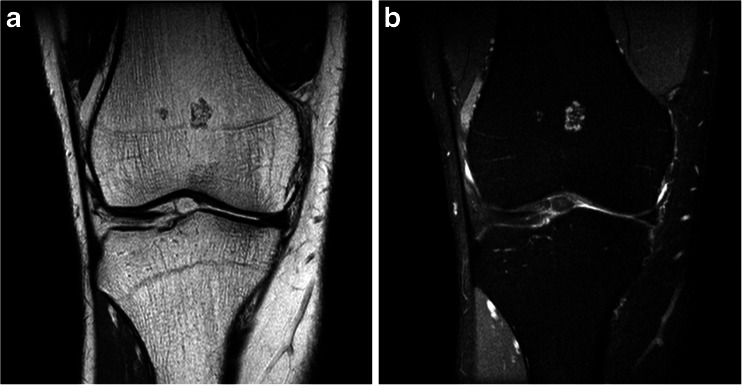
Methods: Participants aged 45 to 65 years were prospectively included, oversampling overweight and obese persons. Within a subgroup of participants, MRI of the right knee was performed and screened for incidental cartilaginous tumours, as defined by their characteristic location and appearance.
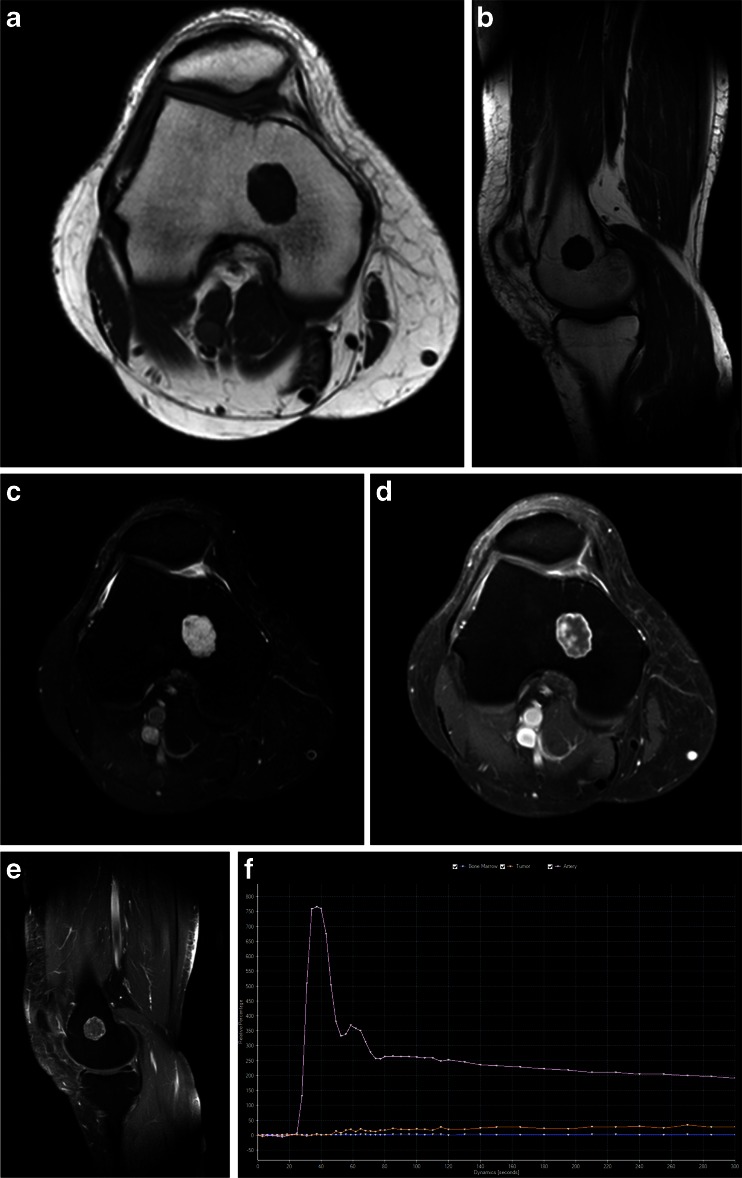
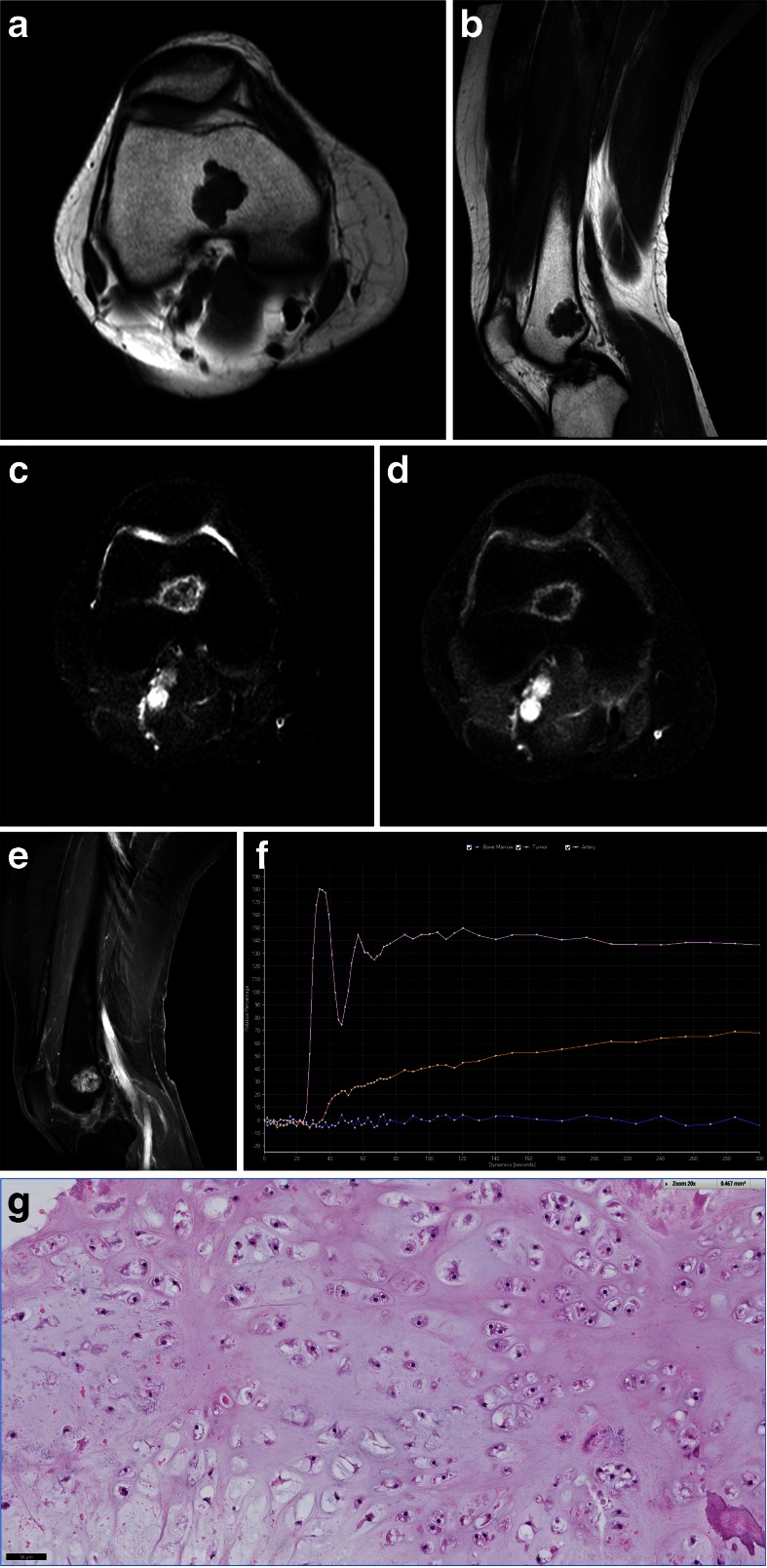
Results: Forty-nine cartilaginous tumours were observed in 44 out of 1285 participants (estimated population prevalence 2.8 %, 95 % CI 2.0-4.0 %). Mean largest tumour diameter was 12 mm (range 2-31 mm). Eight participants with a tumour larger than 20 mm or a tumour with aggressive features were referred to rule out low-grade chondrosarcoma. One was lost to follow-up, three had histologically proven ACT/CS1 and four had dynamic contrast MRI findings consistent with benign enchondroma.
Conclusions: Incidental cartilaginous tumours were relatively common on knee MRI and may be regarded as a normal concurrent finding. However, more tumours than expected were ACT/CS1. Because further examination was performed only when suspicion of chondrosarcoma was high, the actual prevalence might be even higher.
Key points: • Incidental cartilaginous tumours are relatively common on knee MRI. • Most incidental cartilaginous tumours are small and lack suspicious features. • Small cartilaginous tumours without suspicious findings may be a normal concurrent finding. • Large tumours and/or those with suspicious findings should be further investigated. • Atypical cartilaginous tumour/chondrosarcoma grade 1 was found more often than expected.
Keywords: Chondroma; Chondrosarcoma; Incidental findings; Knee; Magnetic resonance imaging.
Figures
References
-
- Milgram JW. The origins of osteochondromas and enchondromas. A histopathologic study. Clin Orthop Relat Res. 1983;174:264–284. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
