

Imaging patients with renal colic-consider ultrasound first
- PMID: 25994497
- PMCID: PMC4519809
- DOI: 10.1007/s13244-015-0396-y
Imaging patients with renal colic-consider ultrasound first
Abstract
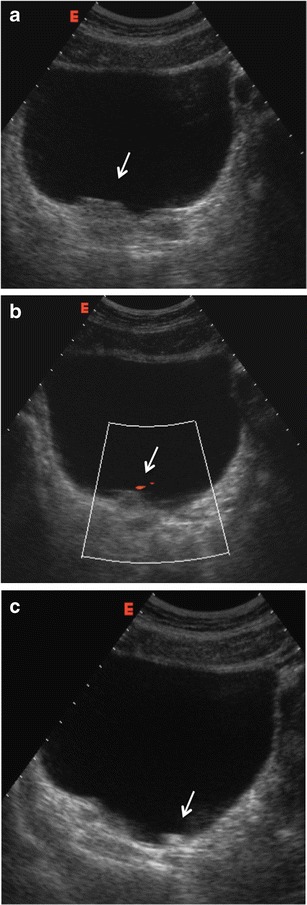
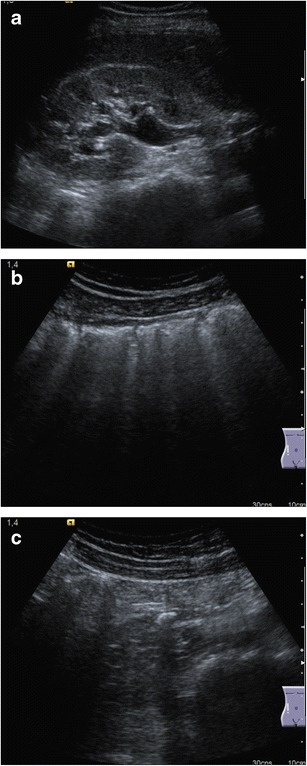
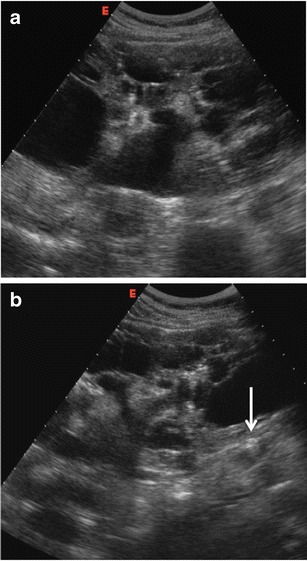
Renal colic is a common disease in Europe and a common cause of visit to the Emergency Department. Clinical diagnosis is usually confirmed by imaging modalities. Unenhanced computed tomography (CT) is considered the best diagnostic test due to its excellent accuracy detecting ureteral stones. However, ultrasound (US) should be considered as the primary imaging technique. It is a reproducible, non-invasive and non-expensive imaging technique, achieving accurate diagnosis in most cases without the need for radiation. Diagnosis is based on the presence of ureteral stones, but indirect findings such as the asymmetry or absence of ureteric jet, an increase of the resistive index or a colour Doppler twinkling artefact may help to suggest the diagnosis when the stone is not identified.
Main messages: • Renal colic diagnosis is usually confirmed by imaging modalities. • Imaging diagnosis of renal colic is based on the detection of ureteral stones. • CT is the most accurate imaging technique to identify ureteral stones. • US allows correct diagnosis in most cases without using radiation. • US should be used as the first imaging modality in patients with renal colic.
Figures

References
LinkOut - more resources
Full Text Sources
Other Literature Sources
