

Effects of Intracoronary Infusion of Escalating Doses of Cardiac Stem Cells in Rats With Acute Myocardial Infarction
- PMID: 25995227
- PMCID: PMC4512882
- DOI: 10.1161/CIRCHEARTFAILURE.115.002210
Effects of Intracoronary Infusion of Escalating Doses of Cardiac Stem Cells in Rats With Acute Myocardial Infarction
Abstract
Background: Although c-kit(pos) cardiac stem cells (CSCs) preserve left ventricular (LV) function and structure after myocardial infarction, CSC doses have been chosen arbitrarily, and the dose-effect relationship is unknown.
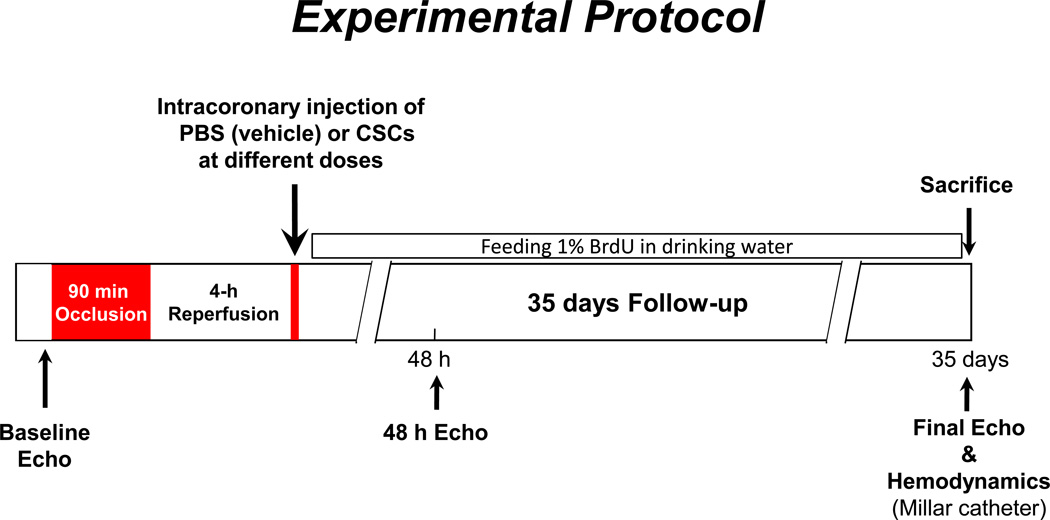
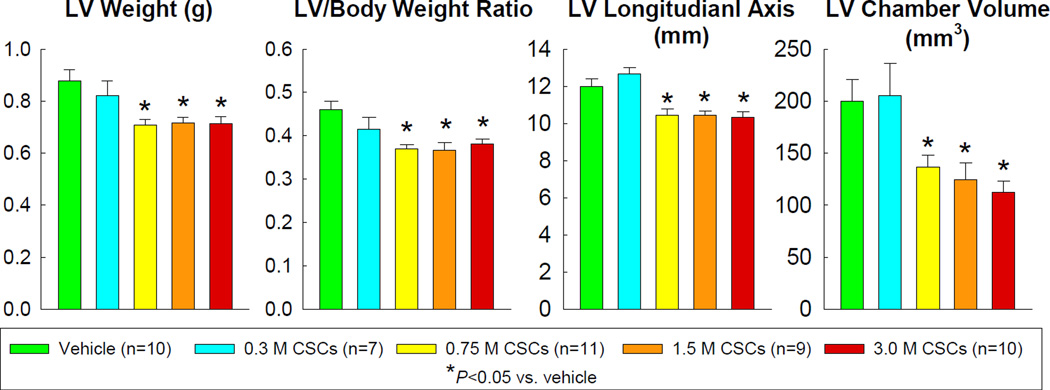
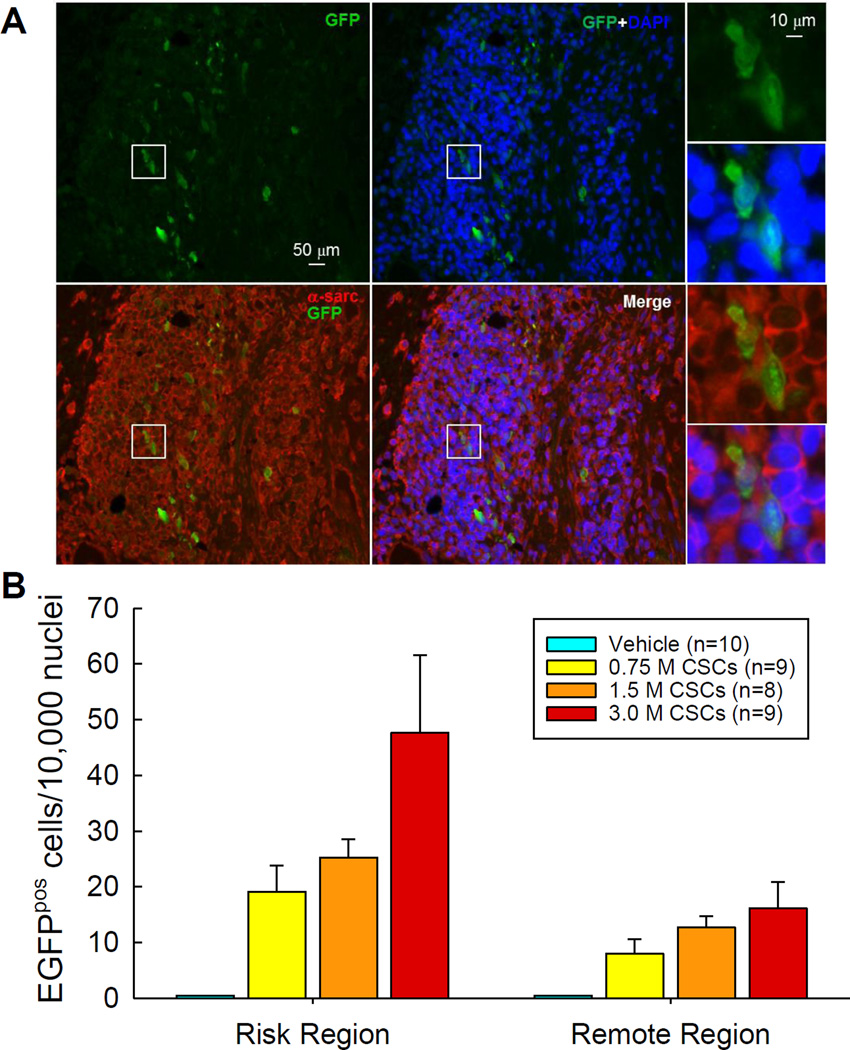
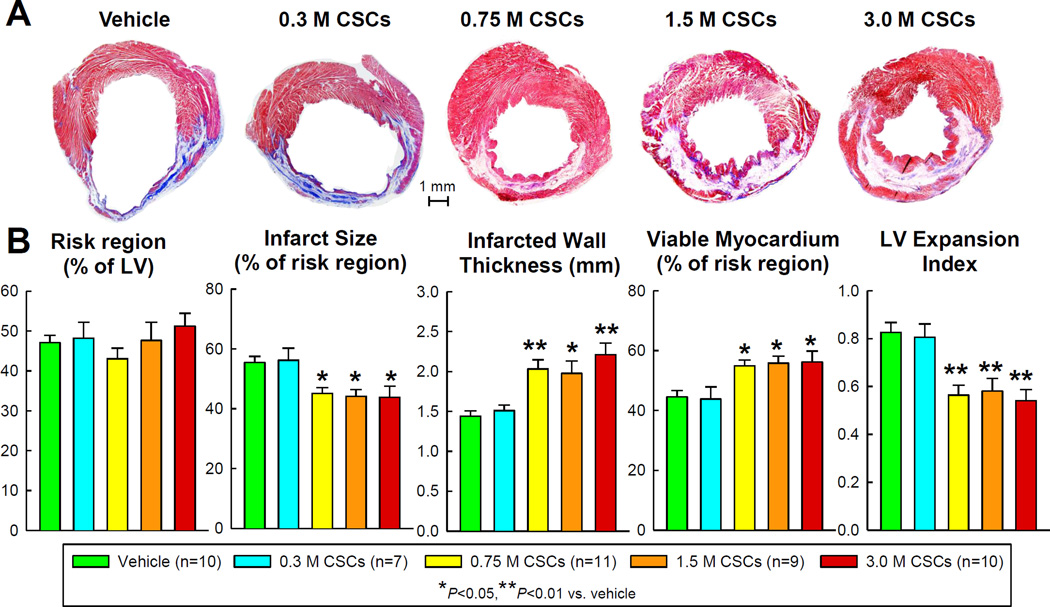
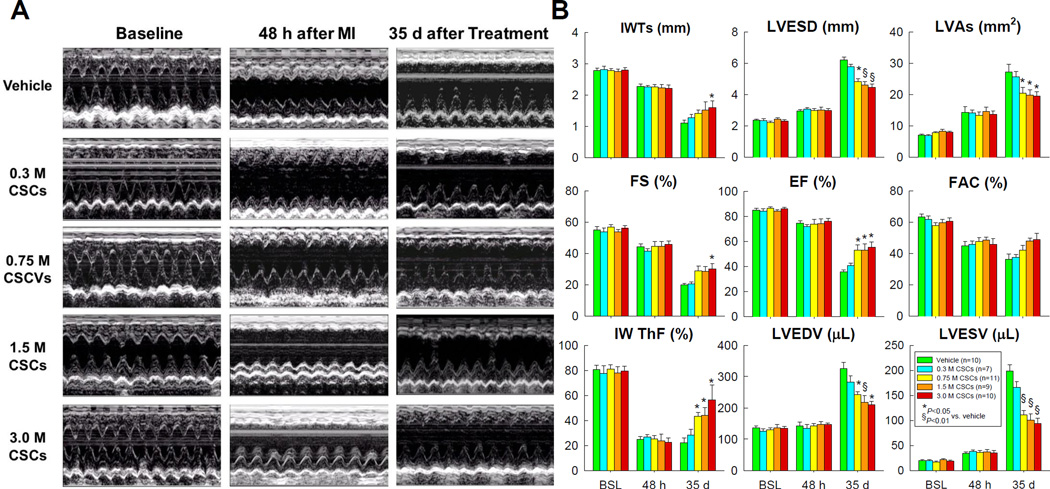
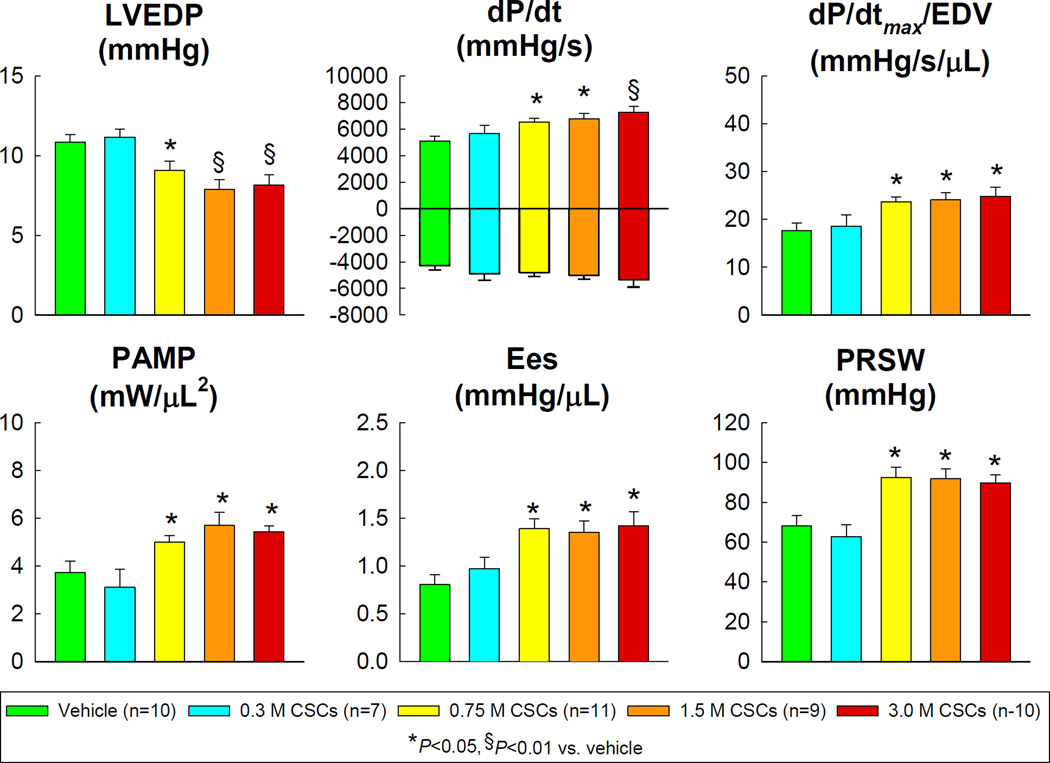
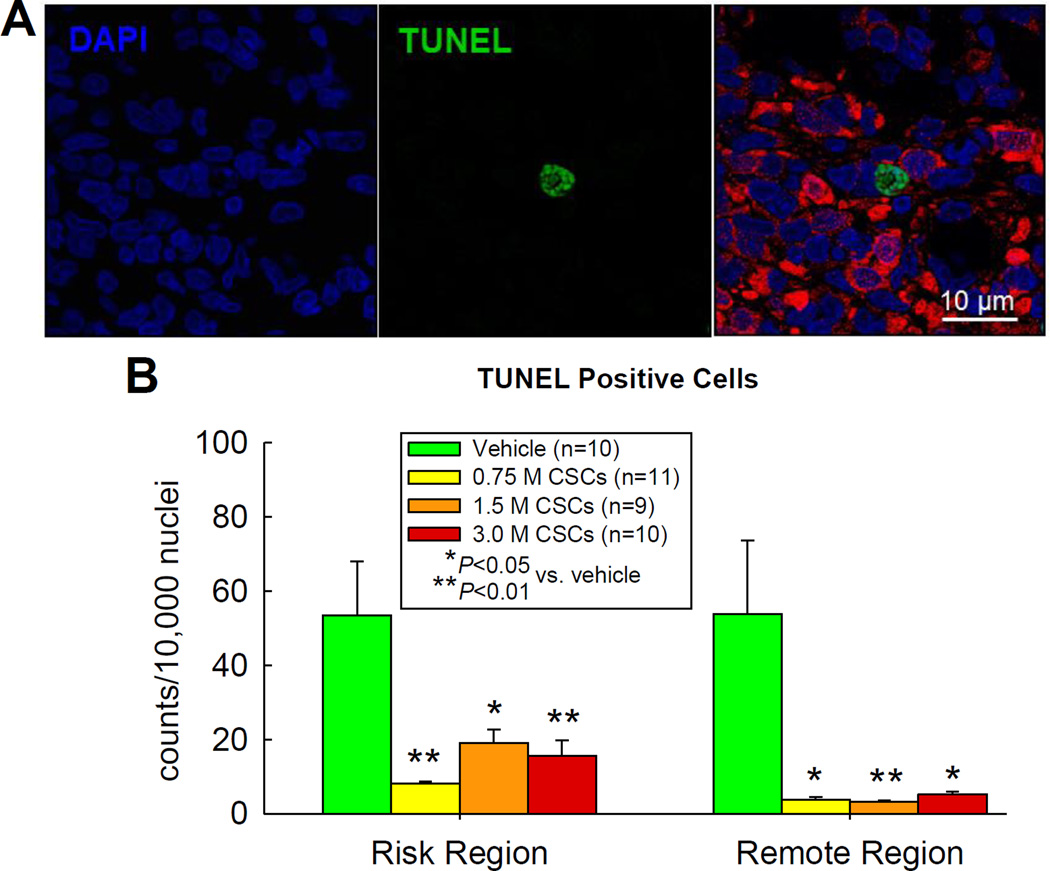
Methods and results: Rats underwent a 90-minute coronary occlusion followed by 35 days of reperfusion. Vehicle or CSCs at 5 escalating doses (0.3×10(6), 0.75×10(6), 1.5×10(6), 3.0×10(6), and 6.0×10(6) cells/heart) were given intracoronarily 4 h after reperfusion. The lowest dose (0.3×10(6)) had no effect on LV function and morphology, whereas 0.75, 1.5, and 3.0×10(6) significantly improved regional and global LV function (echocardiography and hemodynamic studies). These 3 doses had similar effects on echocardiographic parameters (infarct wall thickening fraction, LV end-systolic and end-diastolic volumes, LV ejection fraction) and hemodynamic variables (LV end-diastolic pressure, LV dP/dtmax, preload adjusted maximal power, end-systolic elastance, preload recruitable stroke work) and produced similar reductions in apoptosis, scar size, infarct wall thinning, and LV expansion index and similar increases in viable myocardium in the risk region (morphometry). Infusion of 6.0×10(6) CSCs markedly increased postprocedural mortality. Green fluorescent protein and 5-bromo-2'-deoxyuridine staining indicated that persistence of donor cells and formation of new myocytes were negligible with all doses.
Conclusions: Surprisingly, in this rat model of acute myocardial infarction, the dose-response relationship for intracoronary CSCs is flat. A minimal dose between 0.3 and 0.75×10(6) is necessary for efficacy; above this threshold, a 4-fold increase in cell number does not produce greater improvement in LV function or structure. Further increases in cell dose are harmful.
Keywords: left ventricular function; myocardial infarction; myocardial ischemia; myocardial regeneration; progenitor cells.
© 2015 American Heart Association, Inc.
Figures

References
-
- Beltrami AP, Barlucchi L, Torella D, Baker M, Limana F, Chimenti S, Kasahara H, Rota M, Musso E, Urbanek K, Leri A, Kajstura J, Nadal-Ginard B, Anversa P. Adult cardiac stem cells are multipotent and support myocardial regeneration. Cell. 2003;114:763–776. - PubMed
-
- Bearzi C, Rota M, Hosoda T, Tillmanns J, Nascimbene A, De Angelis A, Yasuzawa-Amano S, Trofimova I, Siggins RW, Lecapitaine N, Cascapera S, Beltrami AP, D'Alessandro DA, Zias E, Quaini F, Urbanek K, Michler RE, Bolli R, Kajstura J, Leri A, Anversa P. Human cardiac stem cells. Proc Natl Acad Sci U S A. 2007;104:14068–14073. - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
