

Planning and guidance of cardiac resynchronization therapy-lead implantation by evaluating coronary venous anatomy assessed with multidetector computed tomography
- PMID: 25995655
- PMCID: PMC4420495
- DOI: 10.4137/CMC.S18762
Planning and guidance of cardiac resynchronization therapy-lead implantation by evaluating coronary venous anatomy assessed with multidetector computed tomography
Abstract
Objectives: We sought to evaluate the utility of multidetector computed tomography (MDCT) in preoperative planning of cardiac resynchronization therapy (CRT) device implantation.
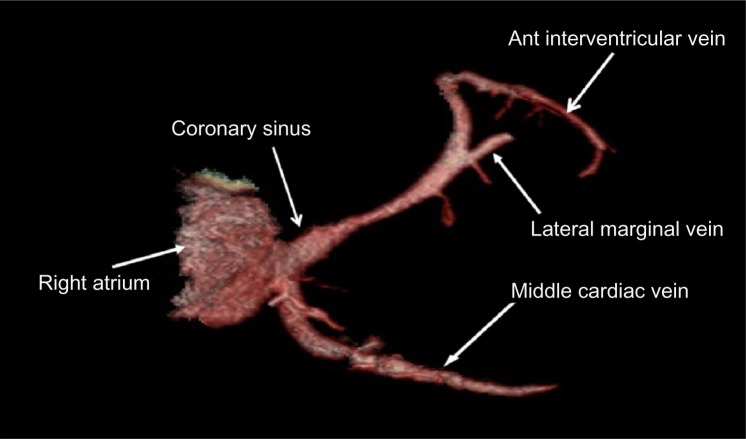
Background: Variation in coronary venous anatomy can affect optimal lead placement and may warrant preimplantation visualization prior to CRT lead placement.
Methods: Prospective randomized enrollment of 29 patients (17 males; mean age at implant 66.7 ± 12.8 years) was undertaken. Patients were randomized to preimplantation MDCT (GE(®) 64-detector Lightspeed, n = 16) or no MDCT. Implantation was planned based on three-dimensional coronary venous reconstruction as visualized in the CT group. Measurement of coronary sinus (CS) angulation, CS ostial (os) diameter, right atrial (RA) width, volume, and height was undertaken prior to implant. Intraoperative CS lead implantation times (introduction, cannulation, and left ventricular [LV] lead positioning), procedure time, fluoroscopy time, and venogram contrast volume were measured to determine if there was a difference between patients who underwent preimplant CT scan and those who did not.
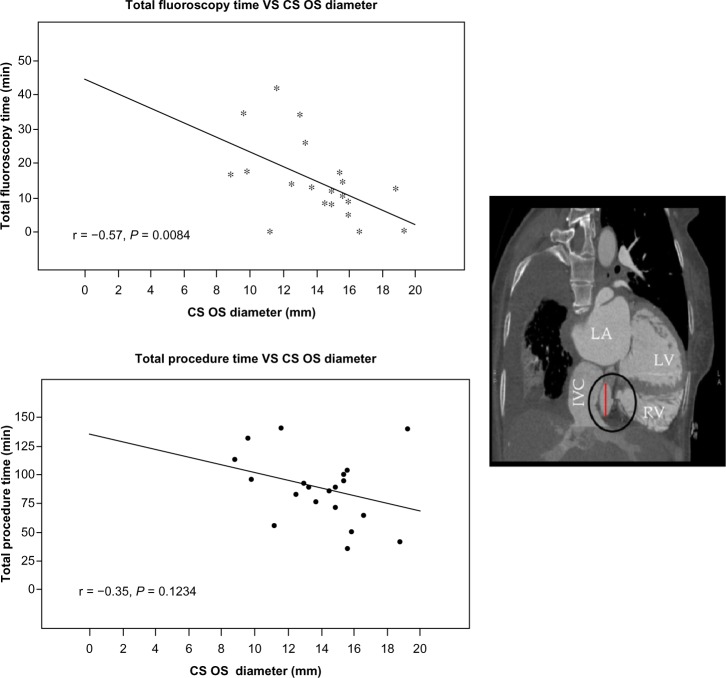
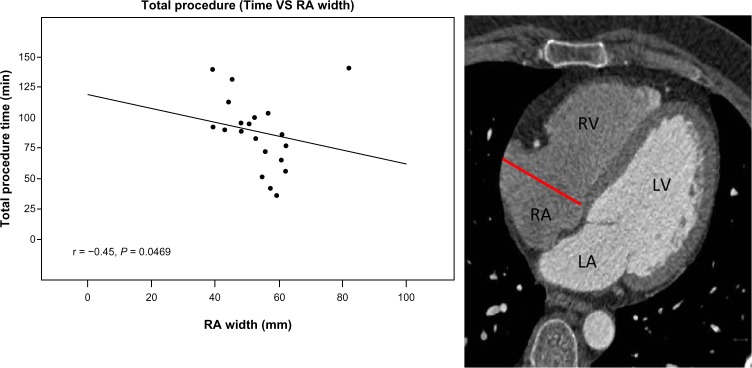
Results: CS os diameter (mean = 13.8 ± 2.9 cm) was inversely correlated with total fluoroscopy time (r = -0.57, P = .008), and total procedure time, but this correlation was not statistically significant (r = -0.36, P = 0.12). RA width (mean = 52.8 ± 9.9 cm) was associated with a shorter total procedure time (r = -0.44, P = .047) and LV lead positioning time (r = -0.33, P = .012). There were no statistically significant differences between the CT group and the non-CT group with respect to total intraoperative and fluoroscopy times or venogram contrast volumes. Total procedure time was longer in the CT group but the difference was not statistically significant (94 ± 27.2 vs. 74.7 ± 26.6; P = .065).
Conclusion: Noninvasive visualization of the coronary venous anatomy before CRT implantation can be used as a guide for lead placement. While no significant differences were noted between the two groups with respect to intraoperative variables, CS os diameter and RA width inversely correlated to a shorter procedure time and LV lead positioning time, respectively. Further clinical trials regarding the utility of MDCT to visualize coronary venous anatomy prior to CRT implantation for procedural planning and lead placement guidance are warranted.
Keywords: cardiac resynchronization therapy; multidetector CT; noninvasive; venous.
Figures
Similar articles
-
Coronary sinus anatomy by computerized tomography, overlaid on live fluoroscopy can be successfully used to guide left ventricular lead implantation: a feasibility study.J Interv Card Electrophysiol. 2013 Apr;36(3):217-22. doi: 10.1007/s10840-012-9736-8. Epub 2012 Nov 30. J Interv Card Electrophysiol. 2013. PMID: 23196855 Clinical Trial.
-
Multimodality imaging for real-time image-guided left ventricular lead placement during cardiac resynchronization therapy implantations.Int J Cardiovasc Imaging. 2019 Jul;35(7):1327-1337. doi: 10.1007/s10554-019-01574-0. Epub 2019 Mar 7. Int J Cardiovasc Imaging. 2019. PMID: 30847659 Free PMC article.
-
Multidetector cardiac tomography: a useful tool before cardiac resynchronization therapy.Cardiol J. 2015;22(5):590-6. doi: 10.5603/CJ.a2015.0011. Epub 2015 Mar 3. Cardiol J. 2015. PMID: 25733321
-
Percutaneous coronary sinus interventions to facilitate implantation of left ventricular lead: a case series and review of literature.J Card Fail. 2012 Apr;18(4):321-9. doi: 10.1016/j.cardfail.2012.01.003. J Card Fail. 2012. PMID: 22464774 Review.
-
Coronary venous system in cardiac computer tomography: Visualization, classification and role.World J Radiol. 2014 Jul 28;6(7):399-408. doi: 10.4329/wjr.v6.i7.399. World J Radiol. 2014. PMID: 25071880 Free PMC article. Review.
Cited by
-
Computed tomography of cardiomyopathies.Cardiovasc Diagn Ther. 2017 Oct;7(5):539-556. doi: 10.21037/cdt.2017.09.07. Cardiovasc Diagn Ther. 2017. PMID: 29255695 Free PMC article. Review.
-
Cardiovascular Imaging: Current Developments in Research and Clinical Practice.Clin Med Insights Cardiol. 2016 Apr 3;8(Suppl 4):57-61. doi: 10.4137/CMC.S38846. eCollection 2014. Clin Med Insights Cardiol. 2016. PMID: 27081320 Free PMC article. No abstract available.
-
The role of cardiac magnetic resonance in identifying appropriate candidates for cardiac resynchronization therapy - a systematic review of the literature.Heart Fail Rev. 2022 Nov;27(6):2095-2118. doi: 10.1007/s10741-022-10263-5. Epub 2022 Aug 31. Heart Fail Rev. 2022. PMID: 36045189
References
-
- Auricchio A, Abraham WT. Cardiac resynchronization therapy: current state of the art. Cost versus benefit. Circulation. 2004;109:300–7. - PubMed
-
- Willerson JT, Kereikaes DJ. Cardiac resynchronization therapy: helpful now in selected patients with CHF. Circulation. 2004;109:308–9. - PubMed
-
- Cleland JGF, Daubert J-C, Erdmann E, et al. Cardiac resynchronization–Heart Failure (CARE-HF) Study Investigators Longer-term effects of cardiac resynchronization therapy on mortality in heart failure [the CArdiac REsynchronization-Heart Failure (CARE-HF) trial extension phase] Eur Heart J. 2006;27(16):1928–32. - PubMed
-
- Go AS, Mozaffarian D, Roger VL, et al. American Heart Association Statistics Committee and Stroke Statistics Subcommittee Executive summary: heart disease and stroke statistics – 2014 update: a report from the American Heart Association. Circulation. 2014;129(3):399–410. - PubMed
-
- Grines CL, Bashore TM, Boudoulas H, Olson S, Shafer P, Wooley CF. Functional abnormalities in isolated left bundle branch block: the effect of interventricular asynchrony. Circulation. 1989;79:845–53. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
