

Association of Choroidal Neovascularization and Central Serous Chorioretinopathy With Optical Coherence Tomography Angiography
- PMID: 25996386
- PMCID: PMC4721607
- DOI: 10.1001/jamaophthalmol.2015.1320
Association of Choroidal Neovascularization and Central Serous Chorioretinopathy With Optical Coherence Tomography Angiography
Abstract
Importance: Choroidal neovascularization (CNV) is a major cause of vision loss in chronic central serous chorioretinopathy (CSCR). Detecting CNV using fluorescein angiography (FA) may be challenging owing to the coexistence of features related to the primary diagnosis of CSCR. Optical coherence tomography angiography (OCTA) allows noninvasive visualization of retinal and choroidal vasculature via motion contrast and may contribute to the unequivocal diagnosis of CNV in this population.
Objective: To evaluate the sensitivity of spectral-domain OCTA in detecting CNV associated with chronic CSCR.
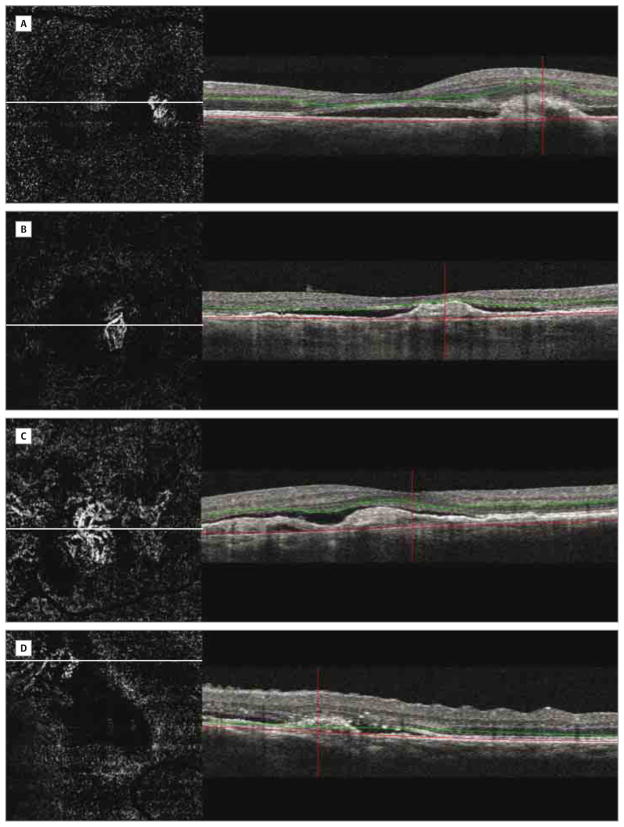
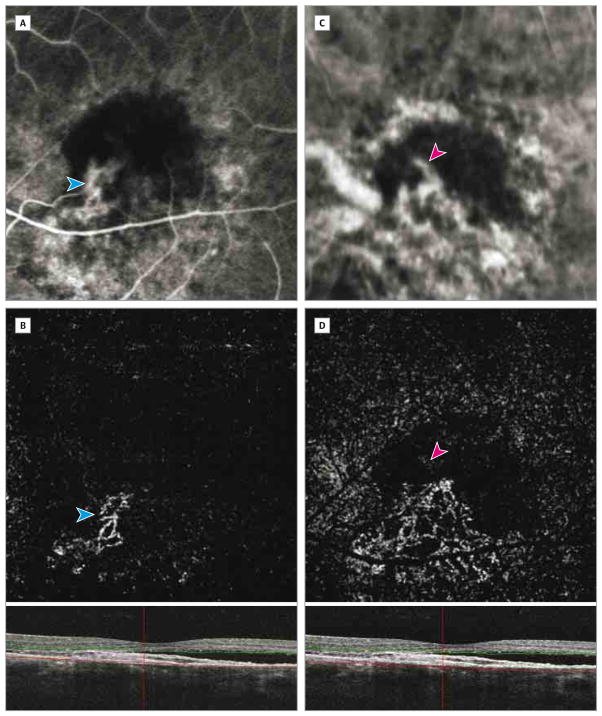
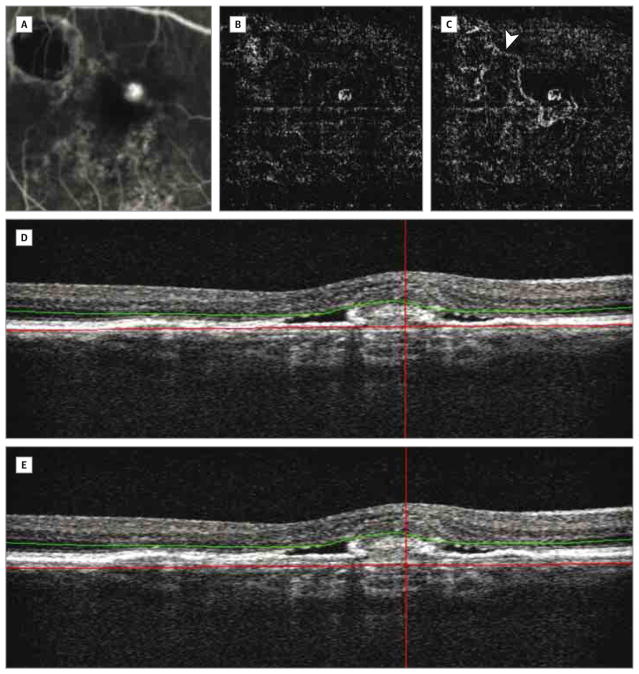
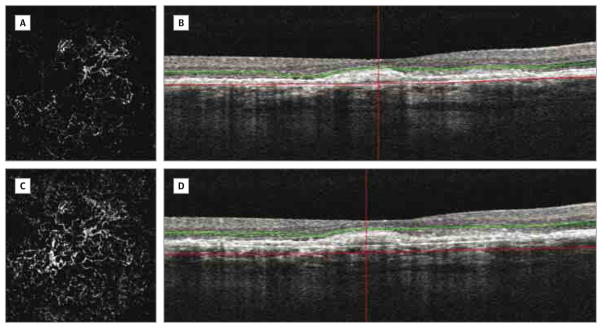
Design, setting, and participants: Observational cross-sectional study including 23 patients (27 eyes) who presented at the New England Eye Center between August 1, 2014, and November 30, 2014, with suspected CNV complicating chronic CSCR and underwent standard assessment for CNV diagnosis, including FA imaging. Participants were prospectively recruited to receive imaging tests using prototype OCTA software on a commercially available spectral-domain OCT. Orthogonal registration and the merging of 2 consecutive image sets were used to obtain 3 × 3-mm and 6 × 6-mm OCT angiograms centered at the macula. Two independent readers masked to other imaging findings performed a qualitative analysis on OCTA depictions of vascular flow representing CNV and the morphologic appearance of CNV.
Main outcomes and measures: Choroidal neovascularization location as well as retinal pigment epithelial detachment internal reflectivity and the presence of subretinal and intraretinal fluid. Sensitivity and specificity of OCTA in detecting CNV were estimated using FA as the standard examination reference.
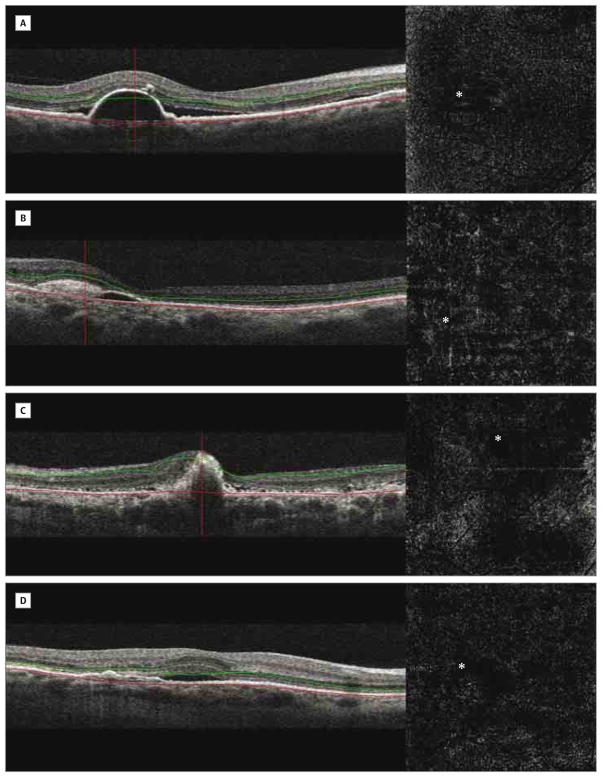
Results: Choroidal neovascularization was diagnosed in 8 of 27 eyes (30%) based on FA imaging analysis. Optical coherence tomography angiography and corresponding OCT B-scans detected 100% (8 of 8) of these CNV lesions and correctly excluded 100% (19 of 19) of eyes with CSCR without CNV. Sensitivity was 100% (95% CI, 0.62-1) and specificity was 100% (95% CI, 0.82-1). Morphologic appearance, location, and position of the CNV relative to the retinal pigment epithelium and Bruch membrane were described using OCTA that combined flow and structural information.
Conclusions and relevance: This study suggests that OCT alone (OCTA and coregistered OCT B-scans) features sensitivity and specificity comparable with FA for the detection of CNV in eyes with chronic CSCR.
Conflict of interest statement
Figures
References
-
- Gomolin JE. Choroidal neovascularization and central serous chorioretinopathy. Can J Ophthalmol. 1989;24(1):20–23. - PubMed
-
- Loo RH, Scott IU, Flynn HW, Jr, et al. Factors associated with reduced visual acuity during long-term follow-up of patients with idiopathic central serous chorioretinopathy. Retina. 2002;22(1):19–24. - PubMed
-
- Spaide RF, Campeas L, Haas A, et al. Central serous chorioretinopathy in younger and older adults. Ophthalmology. 1996;103(12):2070–2079. - PubMed
-
- Gass JD. Photocoagulation treatment of idiopathic central serous choroidopathy. Trans Sect Ophthalmol Am Acad Ophthalmol Otolaryngol. 1977;83(3 pt 1):456–467. - PubMed
-
- Matsunaga H, Nangoh K, Uyama M, Nanbu H, Fujiseki Y, Takahashi K. Occurrence of choroidal neovascularization following photocoagulation treatment for central serous retinopathy [in Japanese] Nihon Ganka Gakkai Zasshi. 1995;99(4):460–468. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
