

High Rates of Asymptomatic, Sub-microscopic Plasmodium vivax Infection and Disappearing Plasmodium falciparum Malaria in an Area of Low Transmission in Solomon Islands
- PMID: 25996619
- PMCID: PMC4440702
- DOI: 10.1371/journal.pntd.0003758
High Rates of Asymptomatic, Sub-microscopic Plasmodium vivax Infection and Disappearing Plasmodium falciparum Malaria in an Area of Low Transmission in Solomon Islands
Abstract
Introduction: Solomon Islands is intensifying national efforts to achieve malaria elimination. A long history of indoor spraying with residual insecticides, combined recently with distribution of long lasting insecticidal nets and artemether-lumefantrine therapy, has been implemented in Solomon Islands. The impact of these interventions on local endemicity of Plasmodium spp. is unknown.
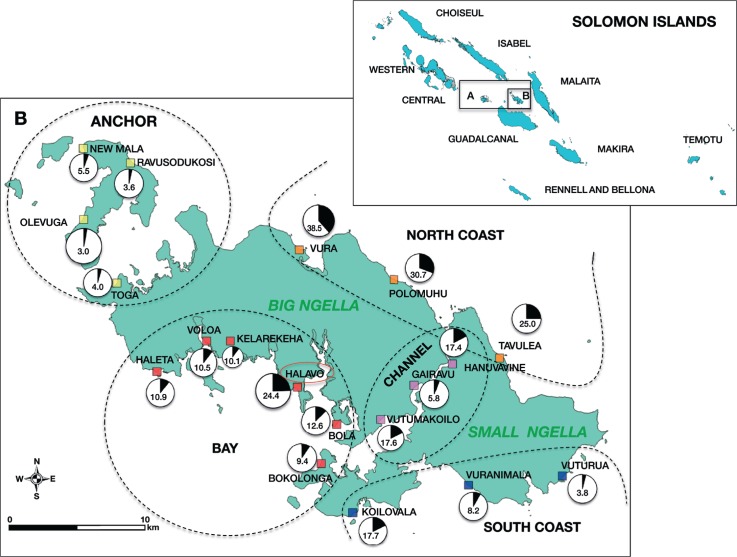
Methods: In 2012, a cross-sectional survey of 3501 residents of all ages was conducted in Ngella, Central Islands Province, Solomon Islands. Prevalence of Plasmodium falciparum, P. vivax, P. ovale and P. malariae was assessed by quantitative PCR (qPCR) and light microscopy (LM). Presence of gametocytes was determined by reverse transcription quantitative PCR (RT-qPCR).
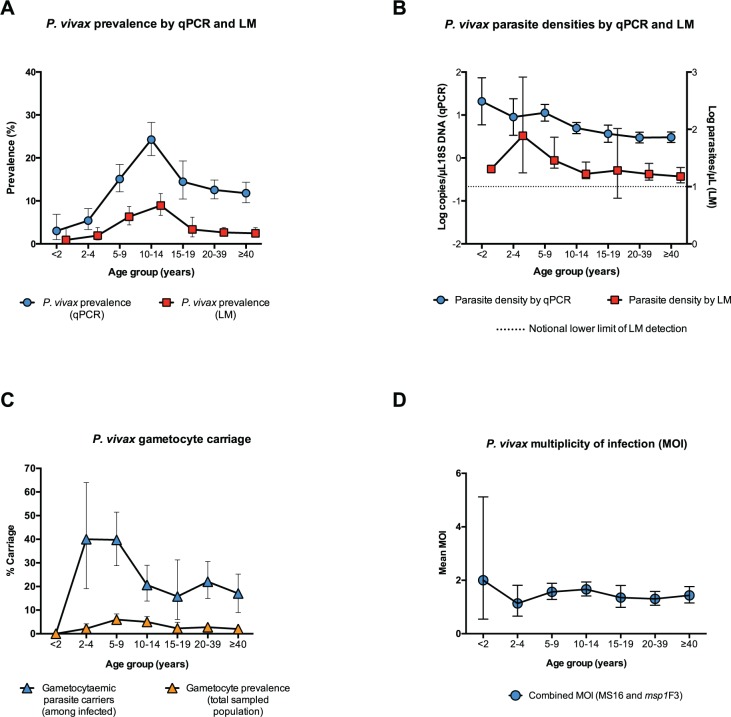
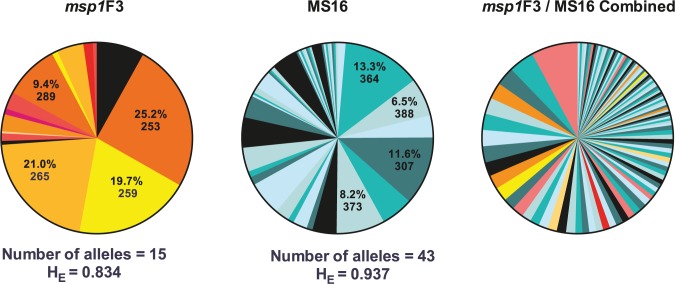
Results: By qPCR, 468 Plasmodium spp. infections were detected (prevalence = 13.4%; 463 P. vivax, five mixed P. falciparum/P. vivax, no P. ovale or P. malariae) versus 130 by LM (prevalence = 3.7%; 126 P. vivax, three P. falciparum and one P. falciparum/P. vivax). The prevalence of P. vivax infection varied significantly among villages (range 3.0-38.5%, p<0.001) and across age groups (5.3-25.9%, p<0.001). Of 468 P. vivax infections, 72.9% were sub-microscopic, 84.5% afebrile and 60.0% were both sub-microscopic and afebrile. Local residency, low education level of the household head and living in a household with at least one other P. vivax infected individual increased the risk of P. vivax infection. Overall, 23.5% of P. vivax infections had concurrent gametocytaemia. Of all P. vivax positive samples, 29.2% were polyclonal by MS16 and msp1F3 genotyping. All five P. falciparum infections were detected in residents of the same village, carried the same msp2 allele and four were positive for P. falciparum gametocytes.
Conclusion: P. vivax infection remains endemic in Ngella, with the majority of cases afebrile and below the detection limit of LM. P. falciparum has nearly disappeared, but the risk of re-introductions and outbreaks due to travel to nearby islands with higher malaria endemicity remains.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Muller I, Bockarie M, Alpers M, Smith T. The epidemiology of malaria in Papua New Guinea. Trends Parasitol. 2003;19(6): 253–9. - PubMed
-
- World Health Organisation (WHO). World Malaria Report 2013. Geneva, Switzerland: World Health Organisation, 2013.
-
- Solomon Islands Vector Borne Disease Control Program (SI NVBDCP). Historical Annual Malaria Records. Honiara, Solomon Islands: Ministry of Health.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
