

Risk Factors for Relapse and Higher Costs Among Medicaid Members with Opioid Dependence or Abuse: Opioid Agonists, Comorbidities, and Treatment History
- PMID: 25997674
- PMCID: PMC4560989
- DOI: 10.1016/j.jsat.2015.05.001
Risk Factors for Relapse and Higher Costs Among Medicaid Members with Opioid Dependence or Abuse: Opioid Agonists, Comorbidities, and Treatment History
Abstract
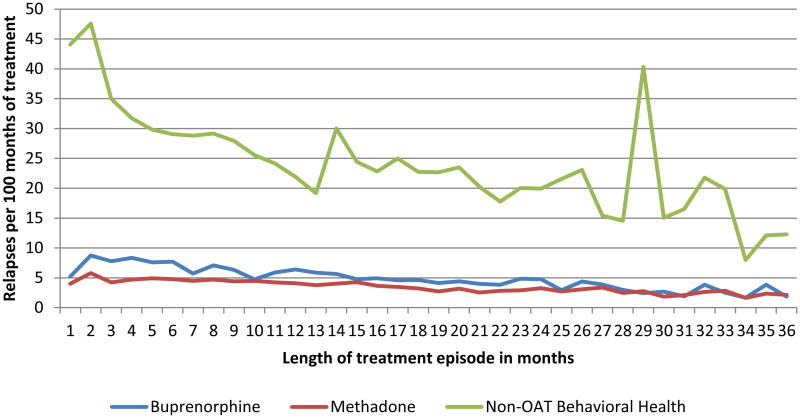
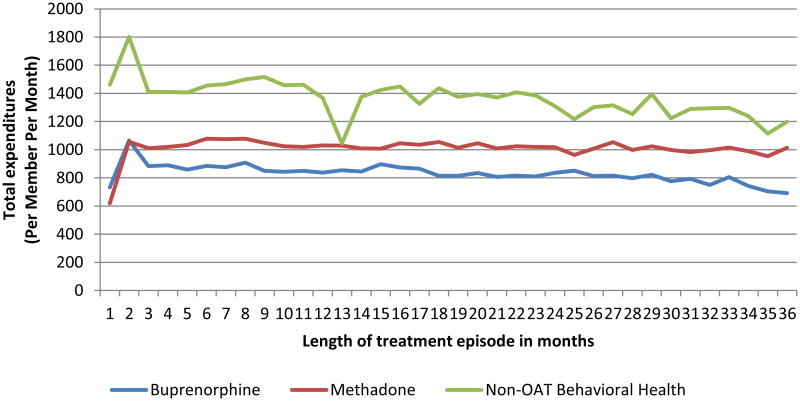
Clinical trials show that opioid agonist therapy (OAT) with methadone or buprenorphine is more effective than behavioral treatments, but state policymakers remain ambivalent about covering OAT for long periods. We used Medicaid claims for 52,278 Massachusetts Medicaid beneficiaries with a diagnosis of opioid abuse or dependence between 2004 and 2010 to study associations between use of methadone, buprenorphine or other behavioral health treatment without OAT, and time to relapse and total healthcare expenditures. Cox Proportional Hazards ratios for patients treated with either methadone or buprenorphine showed approximately 50% lower risk of relapse than behavioral treatment without OAT. Expenditures per month were from $153 to $233 lower for OAT episodes compared to other behavioral treatment. Co-occurring alcohol abuse/dependence quadrupled the risk of relapse, other non-opioid abuse/dependence doubled the relapse risk and severe mental illness added 80% greater risk compared to those without each of those disorders. Longer current treatment episodes were associated with lower risk of relapse. Relapse risk increased as prior treatment exposure increased but prior treatment was associated with slightly lower total healthcare expenditures. These findings suggest that the effectiveness of OAT that has been demonstrated in clinical trials persists at the population level in a less controlled setting and that OAT is associated with lower total healthcare expenditures compared to other forms of behavioral treatment for patients with opioid addiction. Co-occurring other substance use and mental illness exert strong influences on cost and risk of relapse, suggesting that individuals with these conditions need more comprehensive treatment.
Keywords: Buprenorphine; Cost; Economic evaluation; Length of treatment; Medicaid; Methadone; Opioid addiction; Opioid agonists; Public policy; Substance abuse treatment; Treatment history.
Copyright © 2015 Elsevier Inc. All rights reserved.
Figures
References
-
- Baxter JD, Clark RE, Samnaliev M, Leung GY, Hashemi L. Factors Associated with Medicaid Patients' Access to Buprenorphine Treatment. Journal of Substance Abuse Treatment. 2011;41(1):88–96. - PubMed
-
- Cacciola JS, Dugosh KL, Camilleri AC. Treatment history: Relationship to treatment outcomes. Substance use & Misuse. 2009;44:305–321. - PubMed
-
- Clark RE, Baxter JD. Responses of state medicaid programs to buprenorphine diversion: Doing more harm than good? JAMA Internal Medicine. 2013;173(17):1571–1572. - PubMed
-
- Clark RE, Samnaliev M, Baxter JD, Leung GY. The evidence doesn't justify steps by state medicaid programs to restrict opioid addiction treatment with buprenorphine. Health Aff (Millwood) 2011;30(8):1425–1433. - PubMed
-
- Clark RE, Samnaliev M, McGovern MP. Impact of substance disorders on medical expenditures for medicaid beneficiaries with behavioral health disorders. Psychiatric Services. 2009;60(1):35–42. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
