

Is Adult ADHD a Childhood-Onset Neurodevelopmental Disorder? Evidence From a Four-Decade Longitudinal Cohort Study
- PMID: 25998281
- PMCID: PMC4591104
- DOI: 10.1176/appi.ajp.2015.14101266
Is Adult ADHD a Childhood-Onset Neurodevelopmental Disorder? Evidence From a Four-Decade Longitudinal Cohort Study
Abstract
Objective: Despite a prevailing assumption that adult ADHD is a childhood-onset neurodevelopmental disorder, no prospective longitudinal study has described the childhoods of the adult ADHD population. The authors report follow-back analyses of ADHD cases diagnosed in adulthood, alongside follow-forward analyses of ADHD cases diagnosed in childhood, in one cohort.
Method: Participants belonged to a representative birth cohort of 1,037 individuals born in Dunedin, New Zealand, in 1972 and 1973 and followed to age 38, with 95% retention. Symptoms of ADHD, associated clinical features, comorbid disorders, neuropsychological deficits, genome-wide association study-derived polygenic risk, and life impairment indicators were assessed. Data sources were participants, parents, teachers, informants, neuropsychological test results, and administrative records. Adult ADHD diagnoses used DSM-5 criteria, apart from onset age and cross-setting corroboration, which were study outcome measures.
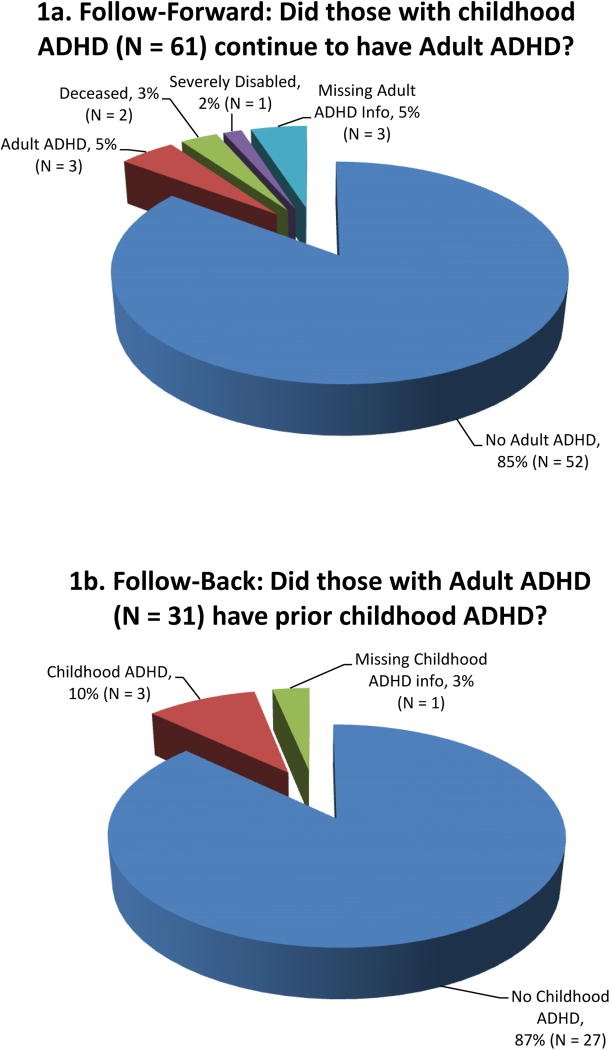
Results: As expected, childhood ADHD had a prevalence of 6% (predominantly male) and was associated with childhood comorbid disorders, neurocognitive deficits, polygenic risk, and residual adult life impairment. Also as expected, adult ADHD had a prevalence of 3% (gender balanced) and was associated with adult substance dependence, adult life impairment, and treatment contact. Unexpectedly, the childhood ADHD and adult ADHD groups comprised virtually nonoverlapping sets; 90% of adult ADHD cases lacked a history of childhood ADHD. Also unexpectedly, the adult ADHD group did not show tested neuropsychological deficits in childhood or adulthood, nor did they show polygenic risk for childhood ADHD.
Conclusions: The findings raise the possibility that adults presenting with the ADHD symptom picture may not have a childhood-onset neurodevelopmental disorder. If this finding is replicated, then the disorder's place in the classification system must be reconsidered, and research must investigate the etiology of adult ADHD.
Conflict of interest statement
Figures
Comment in
-
Is Adult-Onset ADHD a Distinct Entity?Am J Psychiatry. 2015 Oct;172(10):929-31. doi: 10.1176/appi.ajp.2015.15070988. Am J Psychiatry. 2015. PMID: 26423474 No abstract available.
-
Adult Attention-Deficit Hyperactivity Disorder is Being Overdiagnosed.Can J Psychiatry. 2016 Jan;61(1):62. doi: 10.1177/0706743715619938. Can J Psychiatry. 2016. PMID: 27582456 Free PMC article. No abstract available.
References
-
- Cantwell D. Hyperactive children have grown up: What have we learned about what happens to them? Archives of General Psychiatry. 1985;42:1026–8. - PubMed
-
- Barkley RA, Fischer M, Smallish L, Fletcher K. Young adult follow-up of hyperactive children: Antisocial activities and drug use. Journal of Child Psychology & Psychiatry. 2004;45:195–211. - PubMed
-
- Biederman J, Petty CR, Woodworth KY, Lomedico A, Hyder LL, Faraone SV. Adult outcome of attention-deficit/hyperactivity disorder: A controlled 16-year follow-up study. Journal of Clinical Psychiatry. 2012;73:941–50. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
