

Organ donor specimens: What can they tell us about type 1 diabetes?
- PMID: 25998576
- PMCID: PMC4718555
- DOI: 10.1111/pedi.12286
Organ donor specimens: What can they tell us about type 1 diabetes?
Abstract
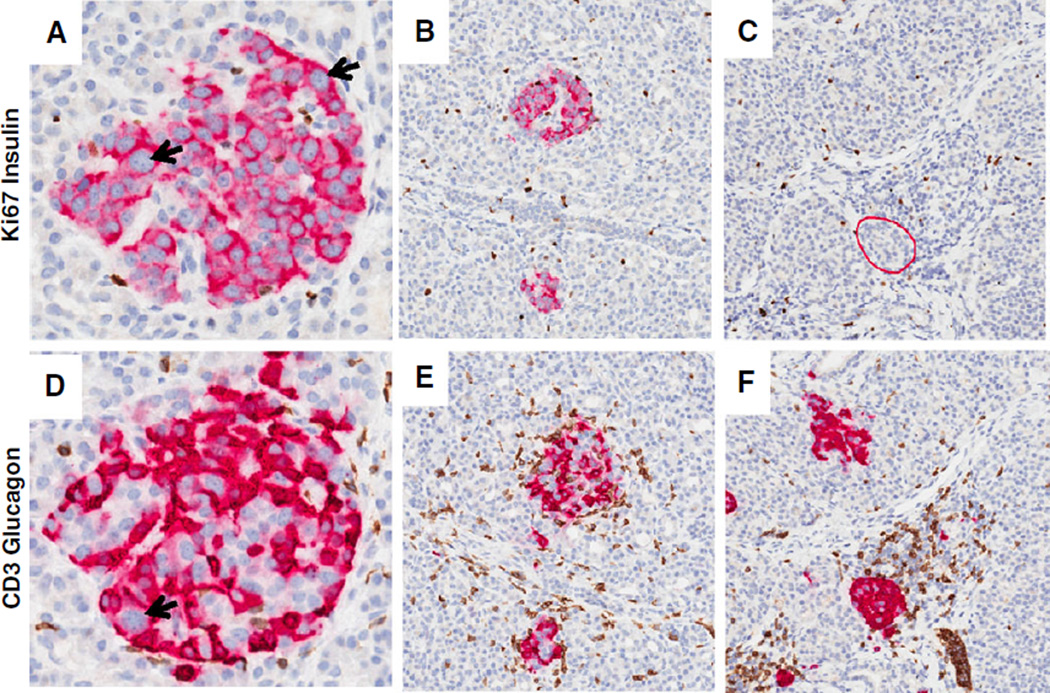
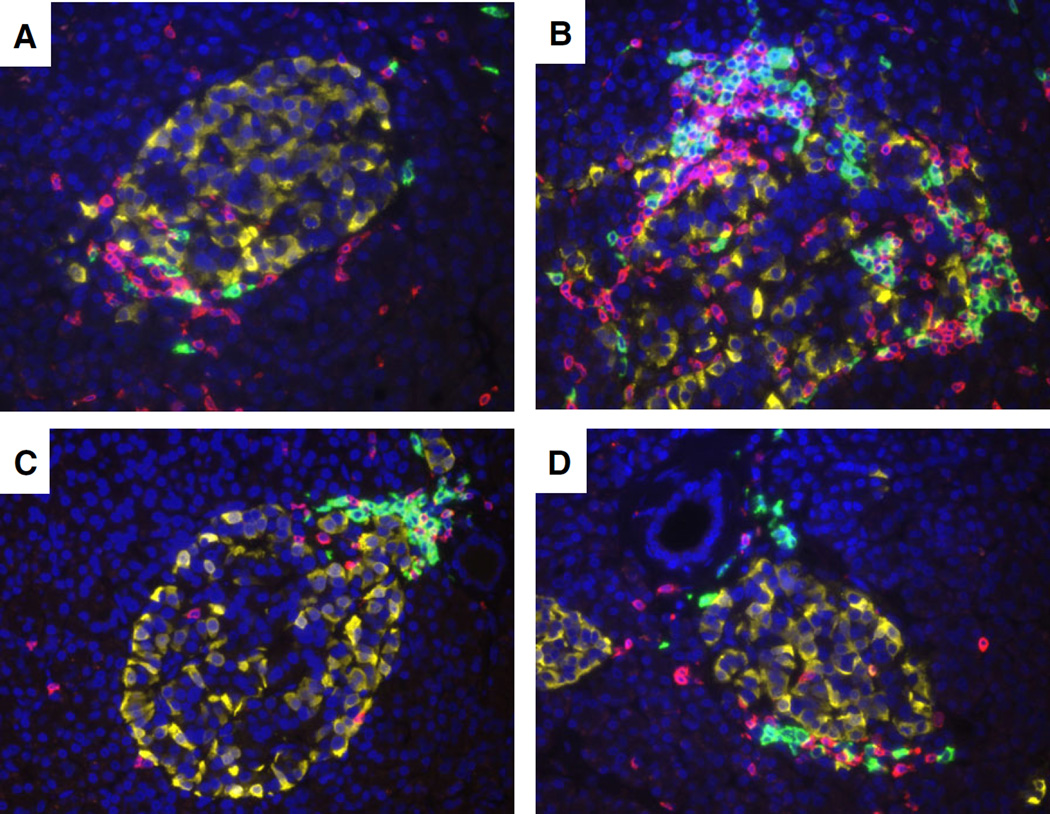
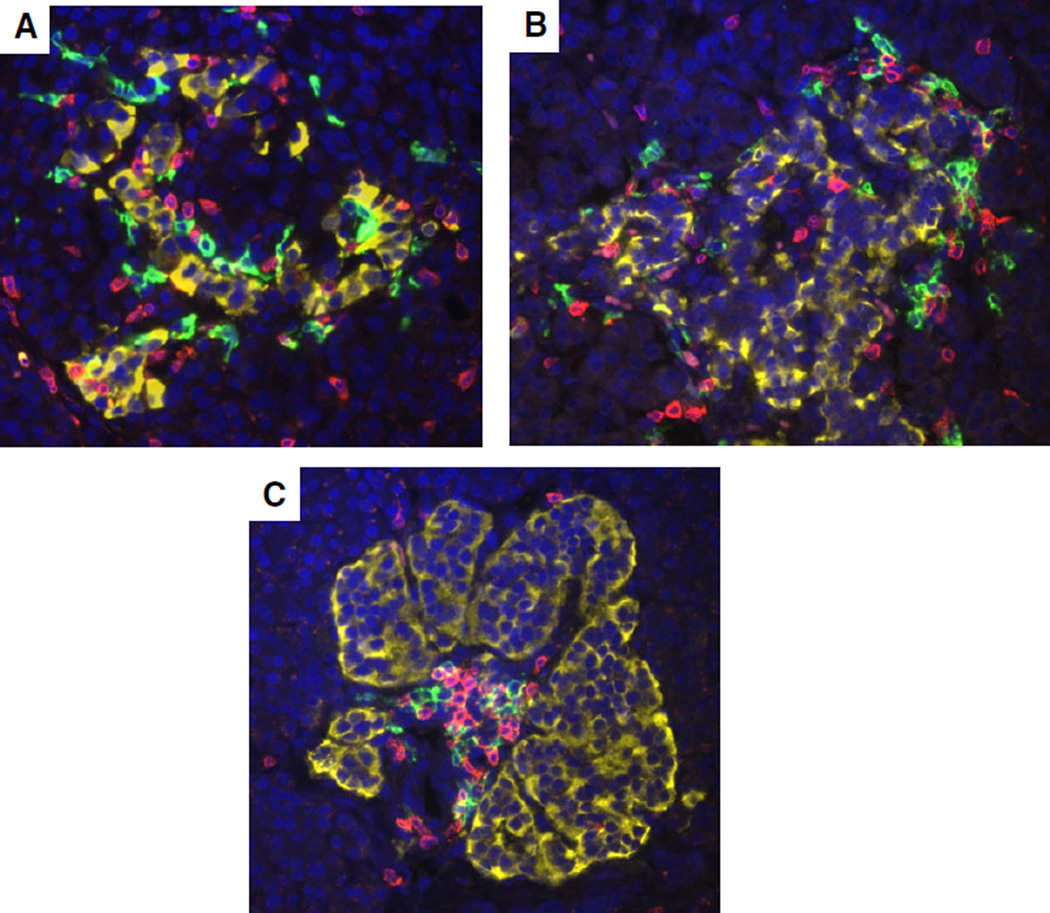
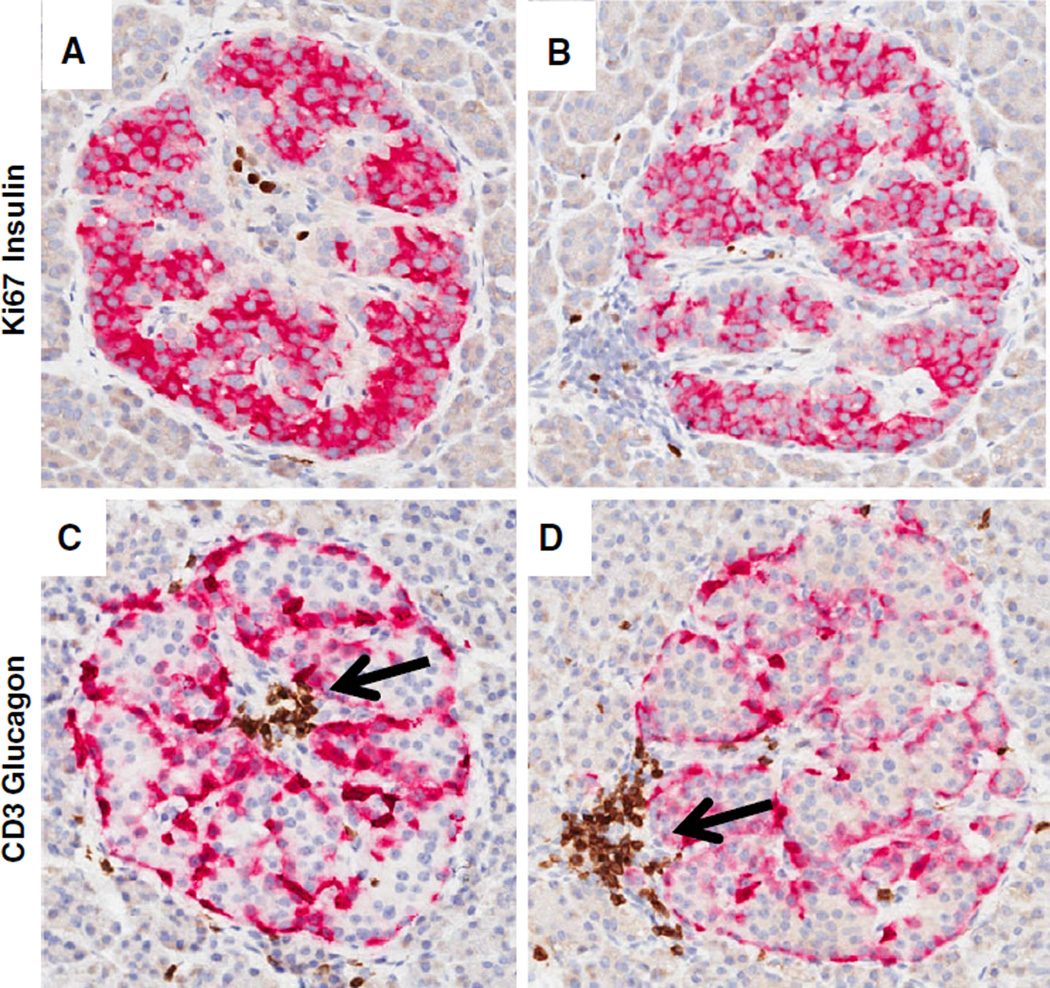
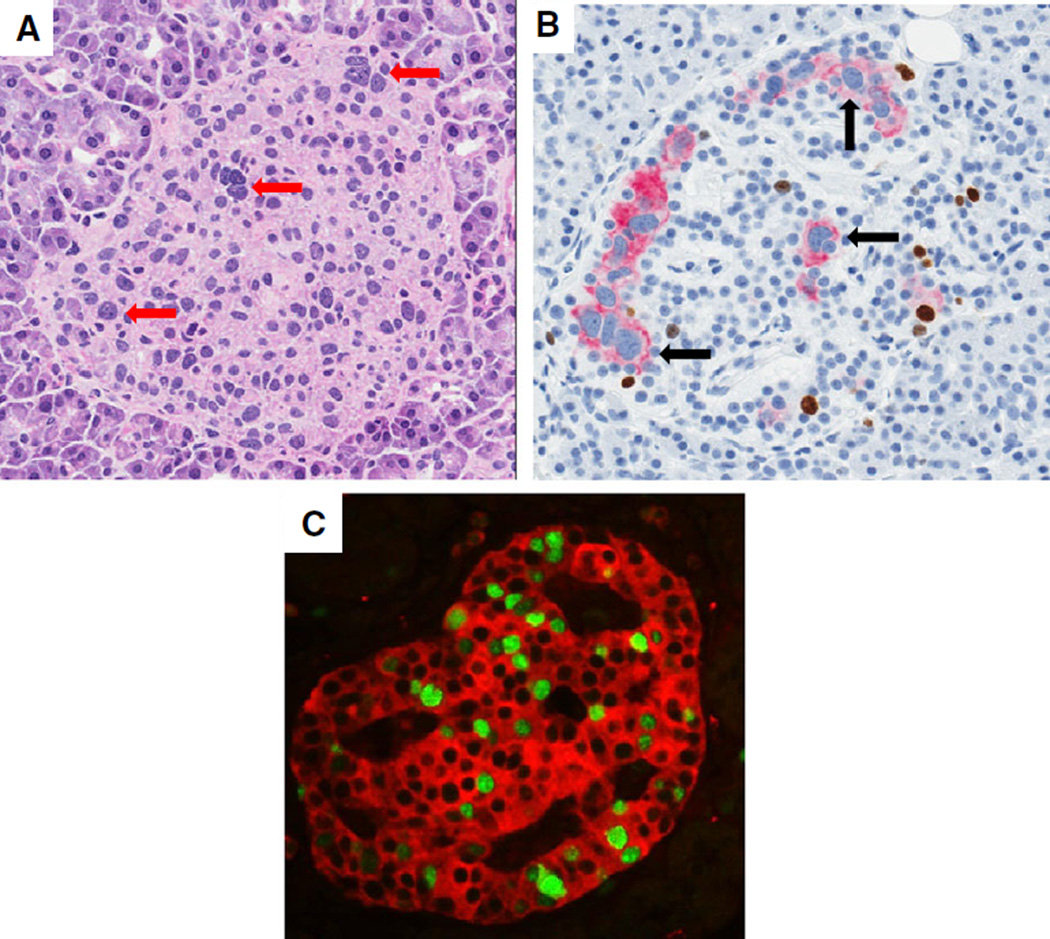
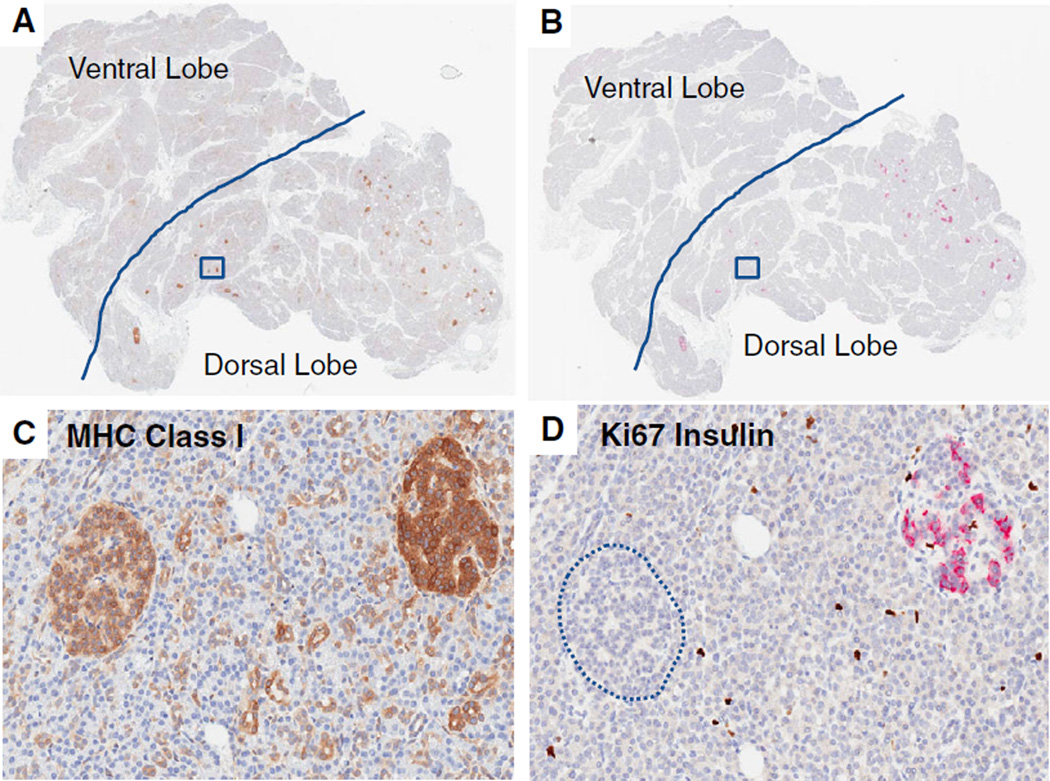
Type 1 diabetes (T1D) is a chronic disease resulting from the destruction of pancreatic beta cells, due to a poorly understood combination of genetic, environmental, and immune factors. The JDRF Network for Pancreatic Organ donors with Diabetes (nPOD) program recovers transplantation quality pancreas from organ donors throughout the USA. In addition to recovery of donors with T1D, non-diabetic donors include those with islet autoantibodies. Donors with type 2 diabetes and other conditions are also recovered to aid investigations directed at the full spectrum of pathophysiological mechanisms affecting beta cells. One central processing laboratory conducts standardized procedures for sample processing, storage, and distribution, intended for current and future cutting edge investigations. Baseline histology characterizations are performed on the pancreatic samples, with images of the staining results provided though whole-slide digital scans. Uniquely, these high-grade biospecimens are provided without expense to investigators, working worldwide, seeking methods for disease prevention and reversal strategies. Collaborative working groups are highly encouraged, bringing together multiple investigators with different expertise to foster collaborations in several areas of critical need. This mini-review will provide some key histopathological findings emanating from the nPOD collection, including the heterogeneity of beta cell loss and islet inflammation (insulitis), beta cell mass, insulin-producing beta cells in chronic T1D, and pancreas weight reductions at disease onset. Analysis of variations in histopathology observed from these organ donors could provide for mechanistic differences related to etiological agents and serve an important function in terms of identifying the heterogeneity of T1D.
Keywords: beta cell; image analysis; insulin; insulitis; islet.
© 2015 John Wiley & Sons A/S. Published by John Wiley & Sons Ltd.
Conflict of interest statement
The author declares no conflict of interest.
Figures
References
-
- Craig ME, Jefferies C, Dabelea D, Balde N, Seth A, Donaghue KC. Definition, epidemiology, and classification of diabetes in children and adolescents. Pediatr Diabetes. 2014;15(Suppl. 20):4–17. - PubMed
-
- Tran F, Stone M, Huang CY, et al. Population-based incidence of diabetes in Australian youth aged 10–18 yr: increase in type 1 diabetes but not type 2 diabetes. Pediatr Diabetes. 2014;15:585–590. - PubMed
-
- Todd JA. Etiology of type 1 diabetes. Immunity. 2010;32:457–467. - PubMed
-
- Malaisse WJ, Maedler K. Imaging of the β-cells of the islets of Langerhans. Diabetes Res Clin Pract. 2012;98:11–18. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
