

Radioimmunotherapy of human tumours
- PMID: 25998714
- PMCID: PMC4798425
- DOI: 10.1038/nrc3925
Radioimmunotherapy of human tumours
Erratum in
- Nat Rev Cancer. 2015 Aug;15(8):509
Abstract
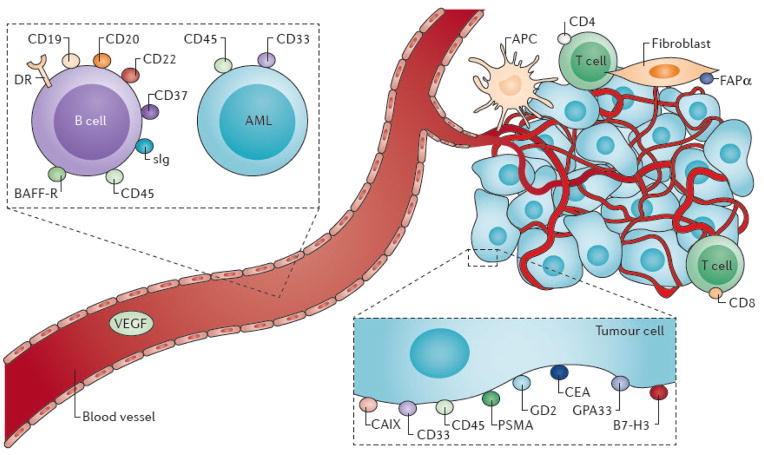
The eradication of cancer remains a vexing problem despite recent advances in our understanding of the molecular basis of neoplasia. One therapeutic approach that has demonstrated potential involves the selective targeting of radionuclides to cancer-associated cell surface antigens using monoclonal antibodies. Such radioimmunotherapy (RIT) permits the delivery of a high dose of therapeutic radiation to cancer cells, while minimizing the exposure of normal cells. Although this approach has been investigated for several decades, the cumulative advances in cancer biology, antibody engineering and radiochemistry in the past decade have markedly enhanced the ability of RIT to produce durable remissions of multiple cancer types.
Conflict of interest statement
There is NO Competing Interest.
Figures
References
-
- Malaise EP, Fertil B, Chavaudra N, Guichard M. Distribution of radiation sensitivities for human tumor cells of specific histological types: comparison of in vitro to in vivo data. Int J Radiat Oncol Biol Phys. 1986;12:617–24. - PubMed
-
- Scott AM, Wolchok JD, Old LJ. Antibody therapy of cancer. Nat Rev Cancer. 2012;12:278–87. Valuable review of general concepts of antigen targets on human tumours and the non-radioactive use of antibodies as therapeutics. - PubMed
-
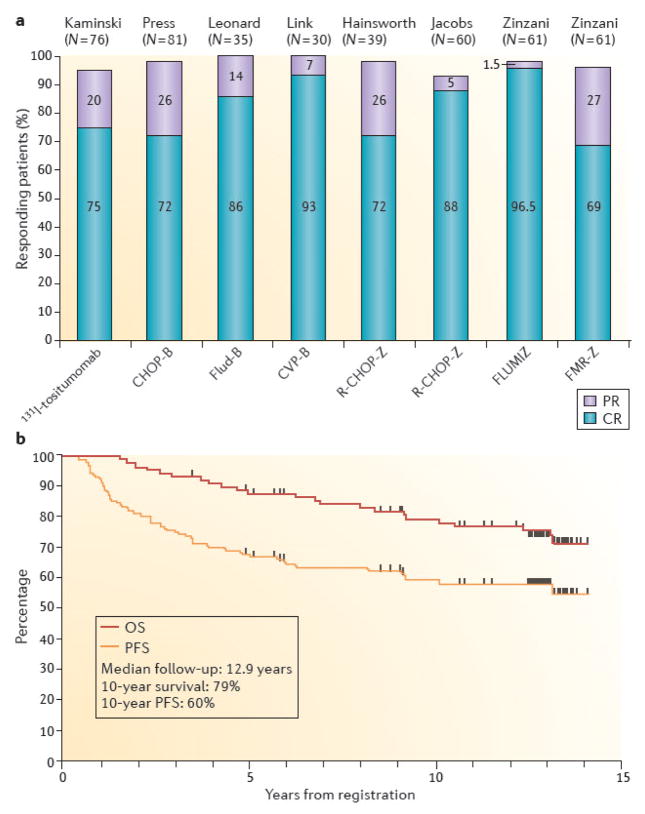
- Kaminski MS, et al. 131I-tositumomab therapy as initial treatment for follicular lymphoma. N Engl J Med. 2005;352:441–9. Benefits of up-front treatment by RIT in lymphoma. - PubMed
-
- Press OW, et al. Radiolabeled-antibody therapy of B-cell lymphoma with autologous bone marrow support. N Engl J Med. 1993;329:1219–24. First demonstration of ability to achieve long-term remission with radioantibodies through RIT in advanced lymphoma. - PubMed
-
- Witzig TE, et al. Treatment with ibritumomab tiuxetan radioimmunotherapy in patients with rituximab-refractory follicular non-Hodgkin's lymphoma. J Clin Oncol. 2002;20:3262–9. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
