

Association between maternal age at childbirth and child and adult outcomes in the offspring: a prospective study in five low-income and middle-income countries (COHORTS collaboration)
- PMID: 25999096
- PMCID: PMC4547329
- DOI: 10.1016/S2214-109X(15)00038-8
Association between maternal age at childbirth and child and adult outcomes in the offspring: a prospective study in five low-income and middle-income countries (COHORTS collaboration)
Abstract
Background: Both young and advanced maternal age is associated with adverse birth and child outcomes. Few studies have examined these associations in low-income and middle-income countries (LMICs) and none have studied adult outcomes in the offspring. We aimed to examine both child and adult outcomes in five LMICs.
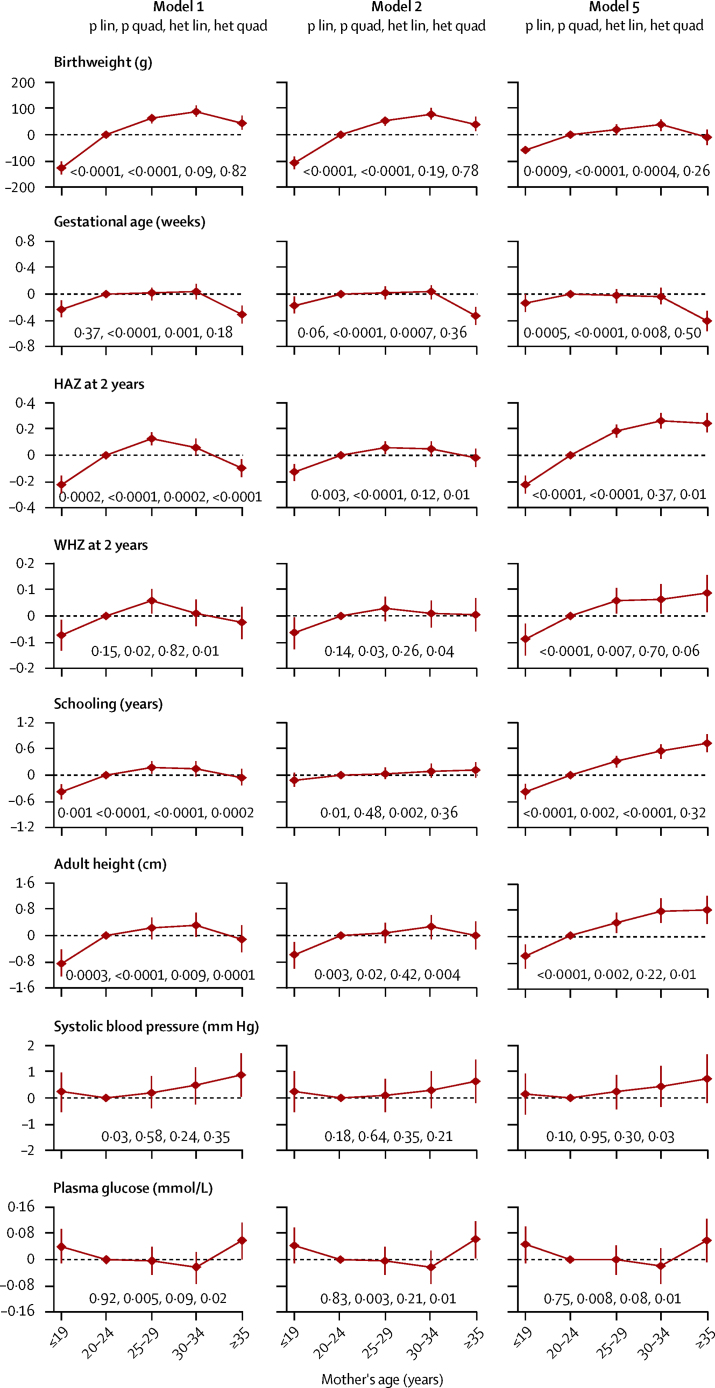
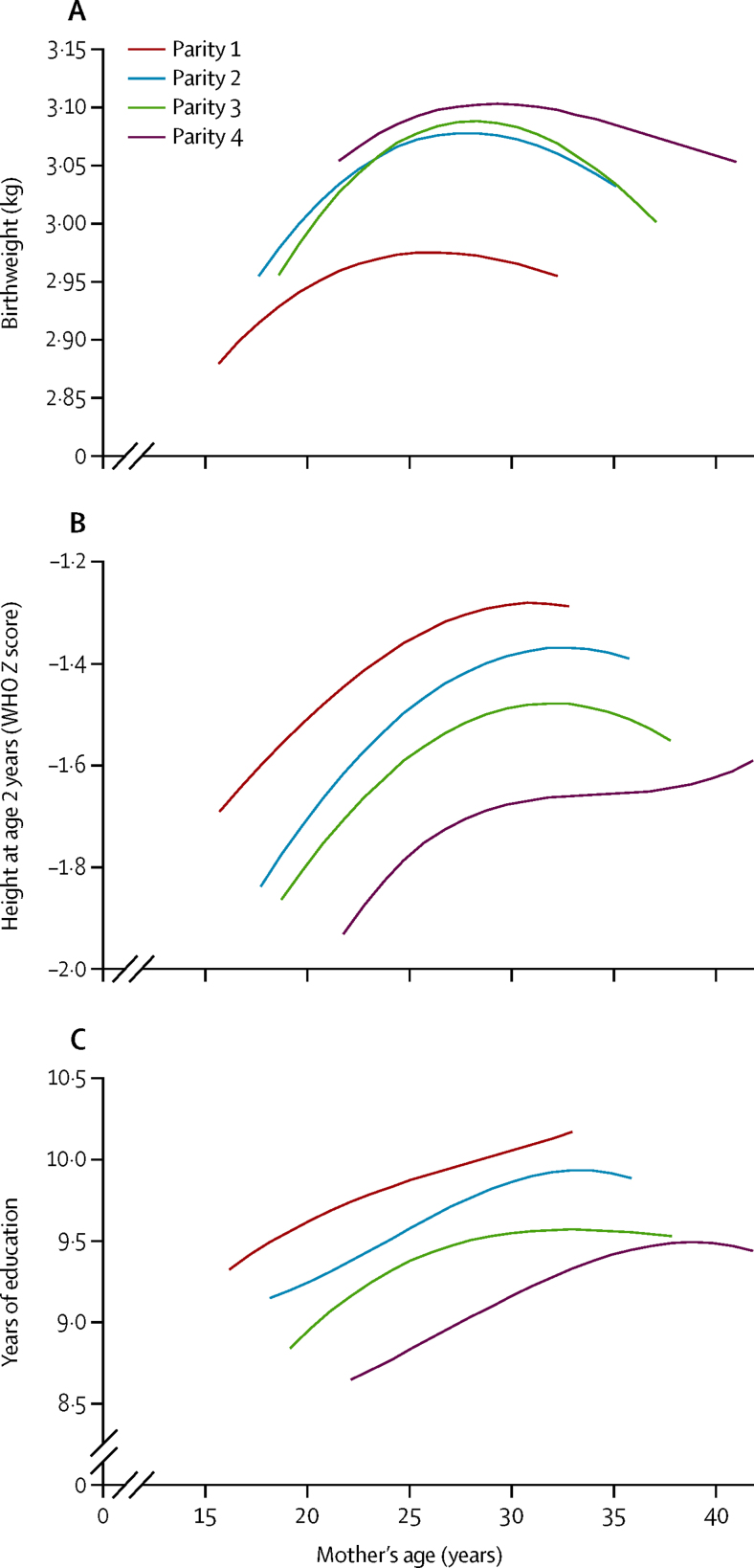
Methods: In this prospective study, we pooled data from COHORTS (Consortium for Health Orientated Research in Transitioning Societies)-a collaboration of five birth cohorts from LMICs (Brazil, Guatemala, India, the Philippines, and South Africa), in which mothers were recruited before or during pregnancy, and the children followed up to adulthood. We examined associations between maternal age and offspring birthweight, gestational age at birth, height-for-age and weight-for-height Z scores in childhood, attained schooling, and adult height, body composition (body-mass index, waist circumference, fat, and lean mass), and cardiometabolic risk factors (blood pressure and fasting plasma glucose concentration), along with binary variables derived from these. Analyses were unadjusted and adjusted for maternal socioeconomic status, height and parity, and breastfeeding duration.
Findings: We obtained data for 22 188 mothers from the five cohorts, enrolment into which took place at various times between 1969 and 1989. Data for maternal age and at least one outcome were available for 19 403 offspring (87%). In unadjusted analyses, younger (≤19 years) and older (≥35 years) maternal age were associated with lower birthweight, gestational age, child nutritional status, and schooling. After adjustment, associations with younger maternal age remained for low birthweight (odds ratio [OR] 1·18 (95% CI 1·02-1·36)], preterm birth (1·26 [1·03-1·53]), 2-year stunting (1·46 [1·25-1·70]), and failure to complete secondary schooling (1·38 [1·18-1·62]) compared with mothers aged 20-24 years. After adjustment, older maternal age remained associated with increased risk of preterm birth (OR 1·33 [95% CI 1·05-1·67]), but children of older mothers had less 2-year stunting (0·64 [0·54-0·77]) and failure to complete secondary schooling (0·59 [0·48-0·71]) than did those with mothers aged 20-24 years. Offspring of both younger and older mothers had higher adult fasting glucose concentrations (roughly 0·05 mmol/L).
Interpretation: Children of young mothers in LMICs are disadvantaged at birth and in childhood nutrition and schooling. Efforts to prevent early childbearing should be strengthened. After adjustment for confounders, children of older mothers have advantages in nutritional status and schooling. Extremes of maternal age could be associated with disturbed offspring glucose metabolism.
Funding: Wellcome Trust and the Bill & Melinda Gates Foundation.
Copyright © 2015 Fall et al. Open access article published under the terms of CC BY. Published by Elsevier Ltd.. All rights reserved.
Figures
Comment in
-
Maternal age matters: for a lifetime, or longer.Lancet Glob Health. 2015 Jul;3(7):e342-3. doi: 10.1016/S2214-109X(15)00034-0. Epub 2015 May 18. Lancet Glob Health. 2015. PMID: 25999095 No abstract available.
-
Disadvantages of having an adolescent mother.Lancet Glob Health. 2016 Nov;4(11):e787-e788. doi: 10.1016/S2214-109X(16)30263-7. Lancet Glob Health. 2016. PMID: 27765286 Free PMC article. No abstract available.
References
-
- Paranjothy S, Broughton H, Adappa R, Fone D. Teenage pregnancy: who suffers? Arch Dis Child. 2009;94:239–245. - PubMed
-
- DuPlessis HM, Bell R, Richards T. Adolescent pregnancy; understanding the impact of age and race on outcomes. J Adolesc Health. 1997;20:187–197. - PubMed
-
- LeGrand TK, Mbacke CS. Teenage pregnancy and child health in the urban Sahel. Stud Fam Plann. 1993;24:137–149. - PubMed
-
- Conde-Agudelo A, Belizan JM, Lammers C. Maternal-perinatal morbidity and mortality associated with adolescent pregnancy in Latin America: cross-sectional survey. Am J Obstet Gynecol. 2005;192:342–349. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
