

Intrauterine synechiae after myomectomy; laparotomy versus laparoscopy: Non-randomized interventional trial
- PMID: 26000007
- PMCID: PMC4426156
Intrauterine synechiae after myomectomy; laparotomy versus laparoscopy: Non-randomized interventional trial
Abstract
Background: Leiomyomata is the most frequent gynecological neoplasm. One of the major complications of myomectomy is intrauterine adhesion (synechiae).
Objective: To evaluate and compare the rate and severity of synechiae formation after myomectomy by laparotomy and laparoscopy.
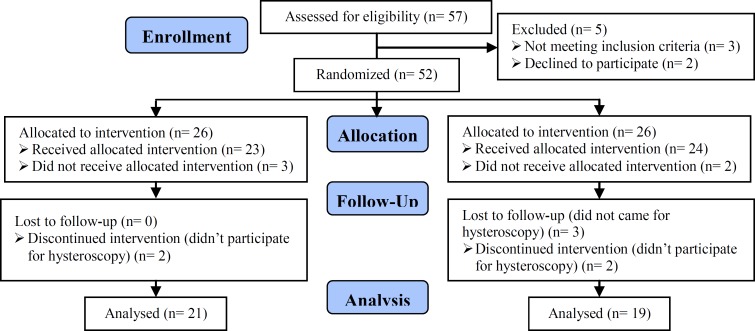
Materials and methods: In this non-randomized interventional trial, hysteroscopy was performed in all married fertile women who had undergone myomectomy (type 3-6 interamural and subserosal fibroids) via laparotomy and laparoscopy in Tehran's Arash Hospital from 2010 to 2013. Three months after the operation, the occurrence rate and severity of intrauterine synechiae, and its relationship with type, number and location of myomas were investigated and compared in both groups.
Results: Forty patients (19 laparoscopy and 21 laparotomy cases) were studied. Both groups were similar regarding the size, type (subserosal or intramural), number and location of myoma. The occurrence rate of synechiae in the laparoscopy and laparotomy group was 21% and 19%, respectively; showing no significant difference (p=0.99). Among all patients, no significant relationship was found between the endometrial opening (p=0.92), location (p=0.14) and type of myoma (p=0.08) with the occurrence rate of synechiae. However, a significant relationship was observed between myoma's size (p=0.01) and the location of the largest myoma with the occurrence of synechiae (p=0.02).
Conclusion: With favorable suturing methods, the outcome of intrauterine synechiae formation after myomectomy, either performed by laparotomy or laparoscopy, is similar. In all cases of myomectomy in reproductive-aged women, postoperative hysteroscopy is highly recommended to better screen intrauterine synechiae.
Keywords: Hysteroscopy; Intrauterine synechiae; Laparoscopy; Laparotomy; Uterine myomectomy.
References
-
- Sami Walid M, Heaton RL. The role of laparoscopic myomectomy in the management of uterine fibroids. Curr Opin Obstet Gynecol. 2011;23:273–277. - PubMed
-
- Cramer SF, Patel A. The frequency of uterine leiomyomas. Am J Clin Pathol. 1990;94:435–438. - PubMed
-
- Buttram VC, Rater RC. Uterine leiomyomata: etiology, symptomatology and management. Fertil Steril. 1981;36:433–445. - PubMed
-
- Olive DL, Lindheim SR, Pritts EA. Non-surgical management of leiomyomata: impact on fertility. Curr Opin Obstet Gynecol. 2004;16:239–243. - PubMed
-
- Lefebvre G AA, Jeffrey J, Vilos G. The management of uterine leiomyomas. SOGC Clinical Practice Guideline No. 128. J Obstet Gynaecol Can. 2003;25:396–405. - PubMed
LinkOut - more resources
Full Text Sources