

Quality of Life in Depressed Patients in UK Primary Care: The FINDER Study
- PMID: 26000214
- PMCID: PMC4389033
- DOI: 10.1007/s40120-013-0006-1
Quality of Life in Depressed Patients in UK Primary Care: The FINDER Study
Abstract
Objectives: To investigate the impact of depression and its treatment on health-related quality of life (HRQoL) in a naturalistic, primary care setting in the UK.
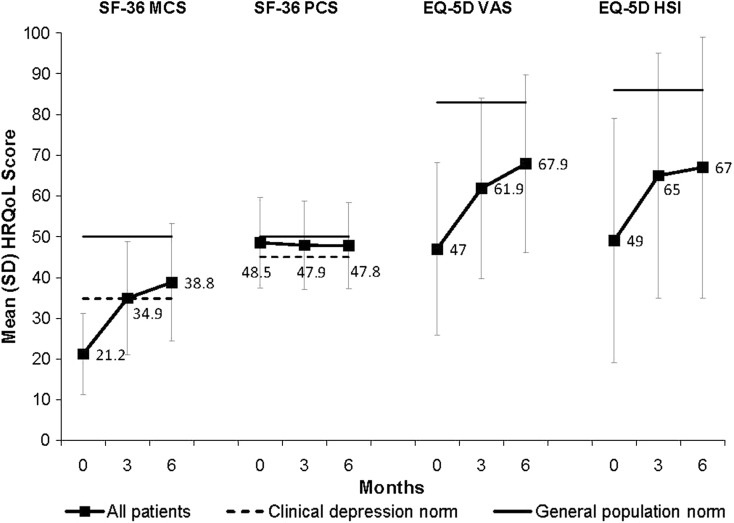
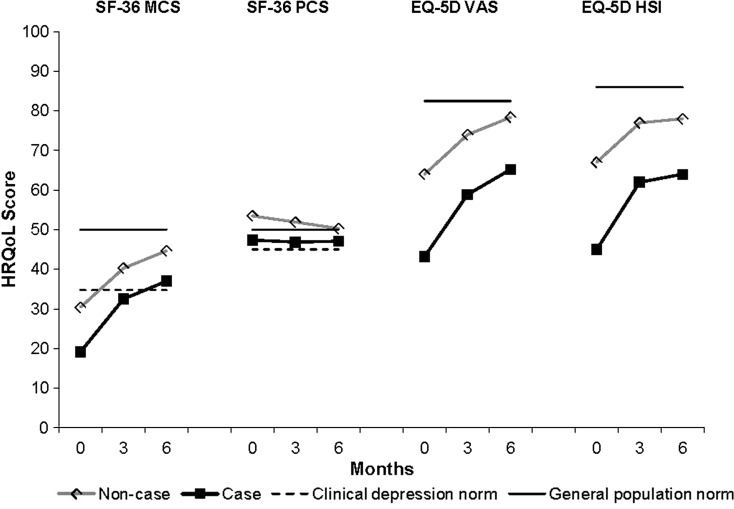
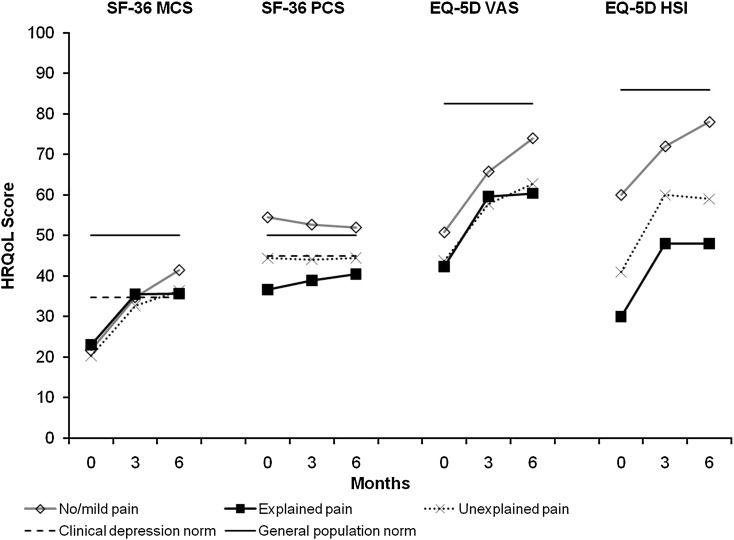
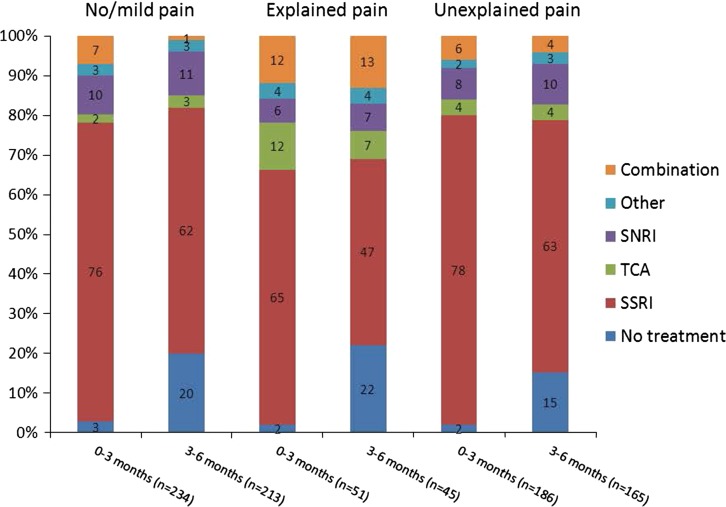
Methods: The Factors Influencing Depression Endpoints Research (FINDER) study was a European, 6-month, prospective, observational study designed to estimate HRQoL in patients with a clinical diagnosis of depression. This paper examines primary care patients recruited in the UK. HRQoL was measured at baseline and at 3 and 6 months after starting antidepressant therapy using the Short Form 36 Health Status Survey and the European Quality of Life-5 Dimensions (EQ-5D). Regression analysis was used to identify baseline and treatment variables independently and significantly associated with HRQoL. Further analyses included the effect of caseness for depression on HRQoL, the effect of moderate/severe pain at baseline on HRQoL, changes in overall pain, pain interference scores, and the use of different antidepressants by pain cohort.
Results: A total of 608 patients was recruited from 58 centres and mean HRQoL was significantly below reported population norms at baseline. Most improvement in HRQoL was seen at 3 months for EQ-5D, with small additional improvement at 6 months. Worse HRQoL outcomes at 6 months were associated with higher somatic symptoms score, duration of depression at baseline, and switching within antidepressant classes. Patients meeting the criteria for caseness for depression, or with significant pain at baseline showed less improvement in HRQoL scores at 6 months.
Conclusion: Patients presenting with depression in primary care show reduced HRQoL compared to population norms. HRQoL improves during antidepressant treatment particularly within the first 3 months. Nonpainful somatic symptoms, socioeconomic factors, depression variables and switching within antidepressant class predict poor HRQoL outcome. Pain is a common symptom in depressed patients and remains after 6 months' treatment. Pain and somatic symptoms should be assessed in all patients with depression in primary care.
Keywords: Antidepressant; Depression; Pain; Primary care; Quality of life.
Figures
References
-
- WHO. Preamble to the Constitution of the World Health Organization as adopted by the International Health Conference, New York, 19–22 June, 1946; signed on 22 July 1946 by the representatives of 61 states (Official Records of the World Health Organization, no. 2, p. 100) and entered into force on 7 April 1948. http://www.who.int/governance/eb/who_constitution_en.pdf. Accessed 14 Feb 2013.
-
- Patrick DL, Erickson P. Health status and health policy: quality of life in health care evaluation and resource allocation. New York: Oxford University Press; 1993.
LinkOut - more resources
Full Text Sources
Other Literature Sources
