

Apnea after Awake Regional and General Anesthesia in Infants: The General Anesthesia Compared to Spinal Anesthesia Study--Comparing Apnea and Neurodevelopmental Outcomes, a Randomized Controlled Trial
- PMID: 26001033
- PMCID: PMC4626294
- DOI: 10.1097/ALN.0000000000000709
Apnea after Awake Regional and General Anesthesia in Infants: The General Anesthesia Compared to Spinal Anesthesia Study--Comparing Apnea and Neurodevelopmental Outcomes, a Randomized Controlled Trial
Abstract
Background: Postoperative apnea is a complication in young infants. Awake regional anesthesia (RA) may reduce the risk; however, the evidence is weak. The General Anesthesia compared to Spinal anesthesia study is a randomized, controlled trial designed to assess the influence of general anesthesia (GA) on neurodevelopment. A secondary aim is to compare rates of apnea after anesthesia.
Methods: Infants aged 60 weeks or younger, postmenstrual age scheduled for inguinal herniorrhaphy, were randomized to RA or GA. Exclusion criteria included risk factors for adverse neurodevelopmental outcome and infants born less than 26 weeks gestation. The primary outcome of this analysis was any observed apnea up to 12 h postoperatively. Apnea assessment was unblinded.
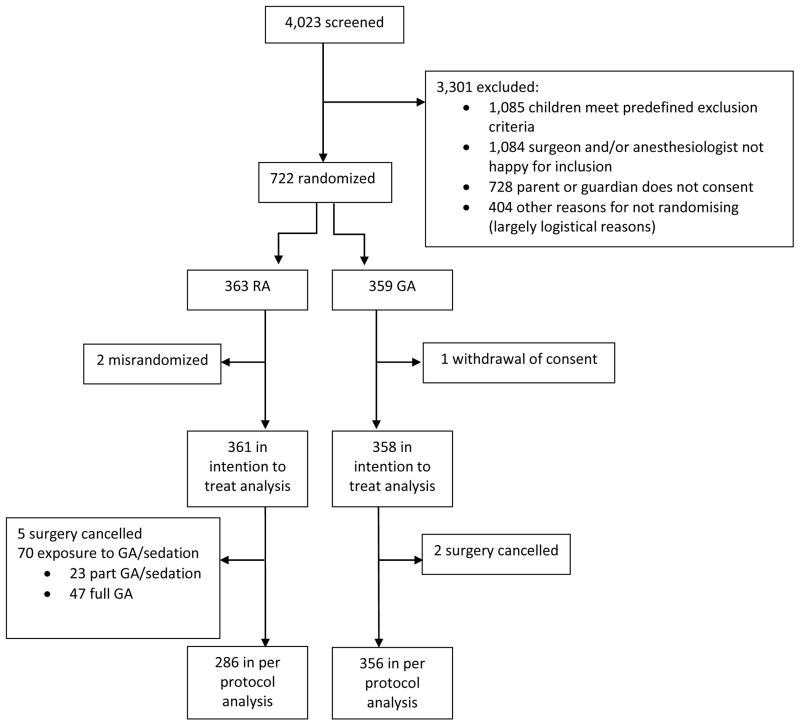
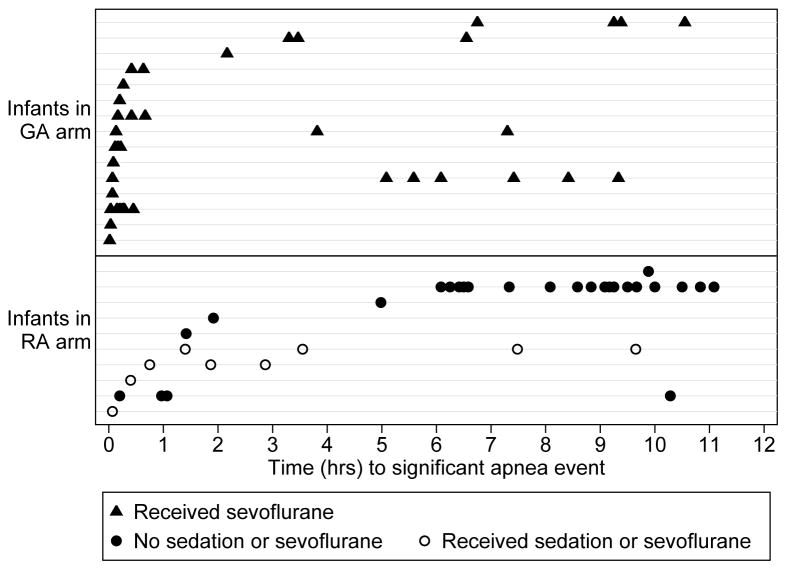
Results: Three hundred sixty-three patients were assigned to RA and 359 to GA. Overall, the incidence of apnea (0 to 12 h) was similar between arms (3% in RA and 4% in GA arms; odds ratio [OR], 0.63; 95% CI, 0.31 to 1.30, P = 0.2133); however, the incidence of early apnea (0 to 30 min) was lower in the RA arm (1 vs. 3%; OR, 0.20; 95% CI, 0.05 to 0.91; P = 0.0367). The incidence of late apnea (30 min to 12 h) was 2% in both RA and GA arms (OR, 1.17; 95% CI, 0.41 to 3.33; P = 0.7688). The strongest predictor of apnea was prematurity (OR, 21.87; 95% CI, 4.38 to 109.24), and 96% of infants with apnea were premature.
Conclusions: RA in infants undergoing inguinal herniorrhaphy reduces apnea in the early postoperative period. Cardiorespiratory monitoring should be used for all ex-premature infants.
Conflict of interest statement
The authors declare no competing interests.
Figures
Comment in
-
Postoperative Apnea in Former Preterm Infants: General Anesthesia or Spinal Anesthesia--Do We Have an Answer?Anesthesiology. 2015 Jul;123(1):15-7. doi: 10.1097/ALN.0000000000000710. Anesthesiology. 2015. PMID: 26001034 No abstract available.
References
-
- Krane EJ, Haberkern CM, Jacobson LE. Postoperative apnea, bradycardia, and oxygen desaturation in formerly premature infants: Prospective comparison of spinal and general anesthesia. Anesth Analg. 1995;80:7–13. - PubMed
-
- Malviya S, Swartx J, Lerman J. Are All Preterm Infants Younger than 60 Weeks Postconceptual Age at Risk for Postanesthetic Apnea? Anesthesiology. 1993;78:1076–81. - PubMed
-
- Cote CJ, Zaslavsky A, Downes JJ, Kurth CD, Welborn LG, Warner LO, Malviya SV. Postoperative Apnea in Former Preterm Infants after Inguinal Herniorrhaphy: A Combined Analysis. Anesthesiology. 1995;82:809–22. - PubMed
-
- Somri M, Gaitini L, Vaida S, Collins G, Sabo E, Mogilner G. Postoperative outcome in high-risk infants undergoing herniorrhaphy: Comparison between spinal and general anaesthesia. Anaesthesia. 1998;53:762–6. - PubMed
-
- Welborn LG, Rice LJ, Hannallah RS, Broadman LM, Ruttimann UE, Fink R. Postoperative Apnea in Former Preterm Infants: Prospective Comparison of Spinal and General Anesthesia. Anesthesiology. 1990;72:838–42. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
