

Long-term outcomes in high-risk patients with non-ST-segment elevation myocardial infarction
- PMID: 26001907
- PMCID: PMC4799793
- DOI: 10.1007/s11239-015-1227-1
Long-term outcomes in high-risk patients with non-ST-segment elevation myocardial infarction
Abstract
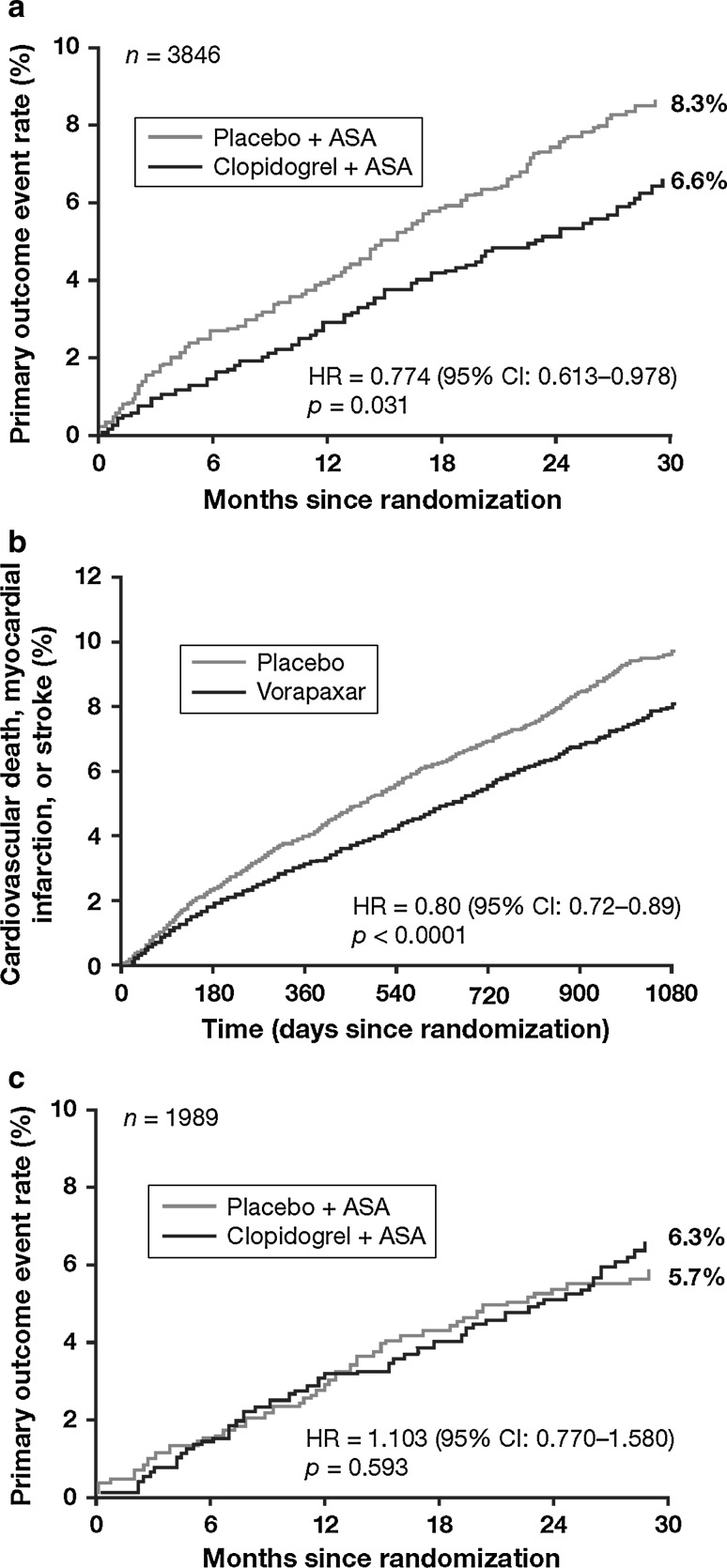
Greater use of evidence-based therapies has improved outcomes for patients with acute coronary syndromes (ACS) in recent decades. Consequently, more ACS patients are surviving beyond 12 months; however, limited data exist to guide treatment in these patients. Long-term outcomes have not improved in non-ST-segment elevation myocardial infarction (NSTEMI) patients at the same rate seen in ST-segment elevation myocardial infarction patients, possibly reflecting NSTEMI patients' more complex clinical phenotype, including older age, greater burden of comorbidities and higher likelihood of a previous myocardial infarction (MI). This complexity impacts clinical decision-making, particularly in high-risk NSTEMI patients, in whom risk-benefit assessments are problematical. This review examines the need for more effective long-term management of NSTEMI patients who survive ≥12 months after MI. Ongoing risk assessment using objective measures of risk (for bleeding and ischemia) should be used in all post-MI patients. While 12 months appears to be the optimal duration of dual antiplatelet therapy for most patients, this may not be the case for high-risk patients, and more research is urgently needed in this population. A recent subgroup analysis from the DAPT study in patients with or without MI who had undergone coronary stenting (31 % presented with MI; 53 % had NSTEMI) and the prospective PEGASUS-TIMI 54 trial in patients with a prior MI and at least one other risk factor (40 % had NSTEMI) demonstrated that long-term dual antiplatelet therapy improved cardiovascular outcomes but increased bleeding. Further studies will help clarify the role of dual antiplatelet therapy in stable post-NSTEMI patients.
Keywords: Acute coronary syndromes; Dual antiplatelet therapy; Non-ST-segment elevation myocardial infarction.
Figures
Similar articles
-
Spontaneous MI After Non-ST-Segment Elevation Acute Coronary Syndrome Managed Without Revascularization: The TRILOGY ACS Trial.J Am Coll Cardiol. 2016 Mar 22;67(11):1289-97. doi: 10.1016/j.jacc.2016.01.034. J Am Coll Cardiol. 2016. PMID: 26988949 Clinical Trial.
-
Predictors of 1-year outcomes in the Taiwan Acute Coronary Syndrome Full Spectrum Registry.J Formos Med Assoc. 2014 Nov;113(11):794-802. doi: 10.1016/j.jfma.2013.08.001. Epub 2013 Sep 26. J Formos Med Assoc. 2014. PMID: 24076272
-
A risk score to predict bleeding in patients with acute coronary syndromes.J Am Coll Cardiol. 2010 Jun 8;55(23):2556-66. doi: 10.1016/j.jacc.2009.09.076. J Am Coll Cardiol. 2010. PMID: 20513595 Clinical Trial.
-
Acute coronary care in the elderly, part I: Non-ST-segment-elevation acute coronary syndromes: a scientific statement for healthcare professionals from the American Heart Association Council on Clinical Cardiology: in collaboration with the Society of Geriatric Cardiology.Circulation. 2007 May 15;115(19):2549-69. doi: 10.1161/CIRCULATIONAHA.107.182615. Circulation. 2007. PMID: 17502590 Review.
-
High-risk non-ST-segment elevation myocardial infarction versus ST-segment elevation myocardial infarction: same behaviour and outcome?J Cardiovasc Med (Hagerstown). 2009 Oct;10 Suppl 1:S13-6. doi: 10.2459/01.JCM.0000362039.48638.92. J Cardiovasc Med (Hagerstown). 2009. PMID: 19851215 Review.
Cited by
-
Impact of Charlson Comorbidity Index on clinical outcomes of patients with non-ST segment elevation acute coronary syndrome: a propensity score matching method.BMJ Open. 2025 Aug 13;15(8):e097359. doi: 10.1136/bmjopen-2024-097359. BMJ Open. 2025. PMID: 40812824 Free PMC article.
-
A comparative study examining the impact of coronary artery bypass grafting surgery with non-extracorporeal circulation on heart function and structure in patients with various forms of coronary heart diseases.Medicine (Baltimore). 2024 Jul 19;103(29):e38844. doi: 10.1097/MD.0000000000038844. Medicine (Baltimore). 2024. PMID: 39029005 Free PMC article.
-
Invasive and antiplatelet treatment of patients with non-ST-segment elevation myocardial infarction: Understanding and addressing the global risk-treatment paradox.Clin Cardiol. 2019 Oct;42(10):1028-1040. doi: 10.1002/clc.23232. Epub 2019 Jul 17. Clin Cardiol. 2019. PMID: 31317575 Free PMC article. Review.
-
Dropping risk stratification with subsequent treatment-risk paradox in non ST elevation acute coronary syndromes: a clinical audit in Iraq.BMC Health Serv Res. 2021 Sep 26;21(1):1015. doi: 10.1186/s12913-021-07034-7. BMC Health Serv Res. 2021. PMID: 34565377 Free PMC article.
-
Poor long-term outcome in acute coronary syndrome in a real-life setting: Ten-year outcome of the TACOS study.Cardiol J. 2021;28(2):302-311. doi: 10.5603/CJ.a2019.0037. Epub 2019 Apr 17. Cardiol J. 2021. PMID: 30994181 Free PMC article.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
