

Healthcare use for acute gastrointestinal illness in two Inuit communities: Rigolet and Iqaluit, Canada
- PMID: 26001982
- PMCID: PMC4441732
- DOI: 10.3402/ijch.v74.26290
Healthcare use for acute gastrointestinal illness in two Inuit communities: Rigolet and Iqaluit, Canada
Abstract
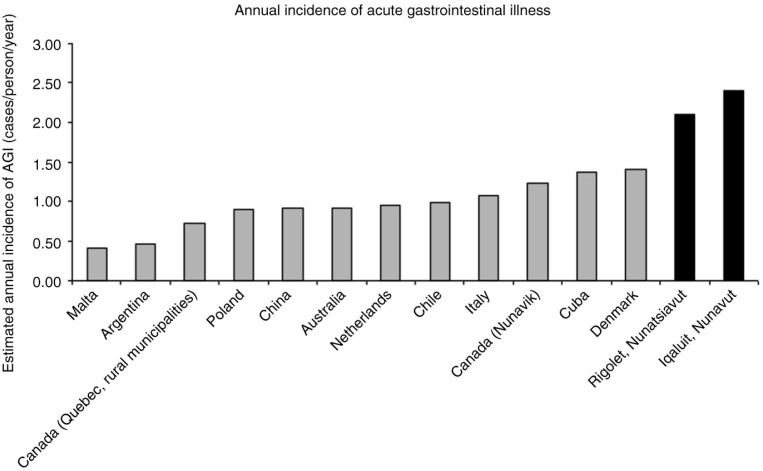
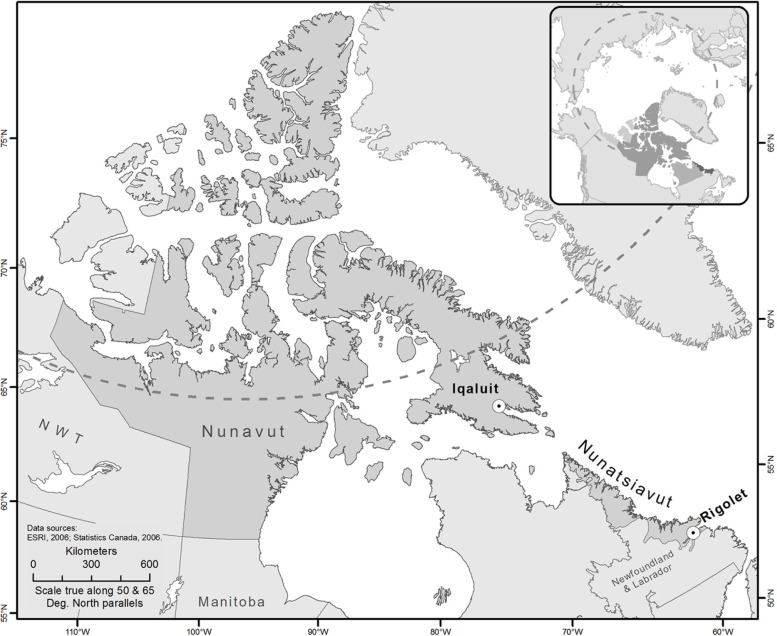
Background: The incidence of self-reported acute gastrointestinal illness (AGI) in Rigolet, Nunatsiavut, and Iqaluit, Nunavut, is higher than reported elsewhere in Canada; as such, understanding AGI-related healthcare use is important for healthcare provision, public health practice and surveillance of AGI.
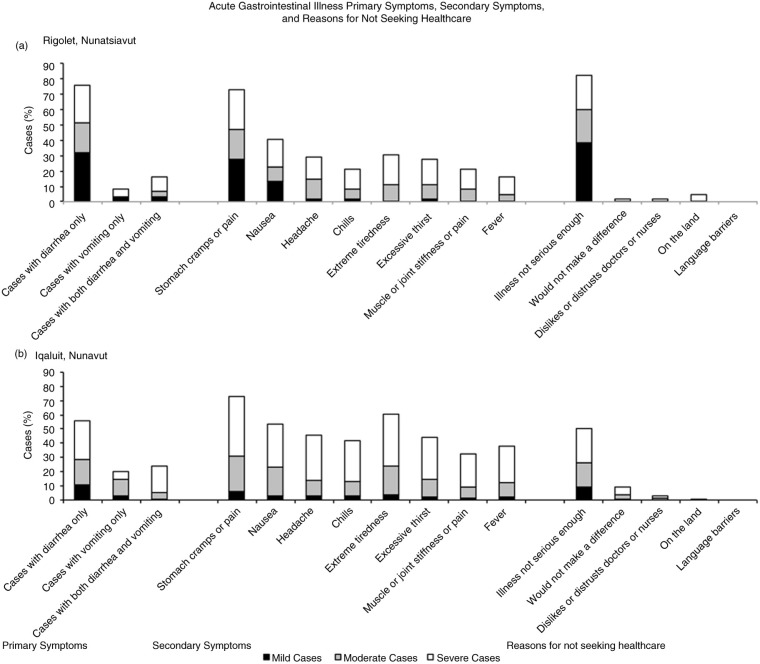
Objectives: This study described symptoms, severity and duration of self-reported AGI in the general population and examined the incidence and factors associated with healthcare utilization for AGI in these 2 Inuit communities.
Design: Cross-sectional survey data were analysed using multivariable exact logistic regression to examine factors associated with individuals' self-reported healthcare and over-the-counter (OTC) medication utilization related to AGI symptoms.
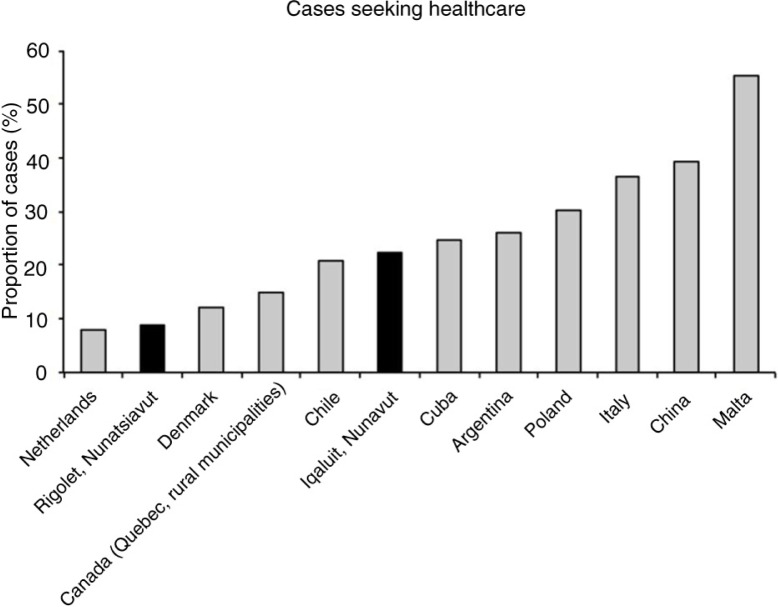
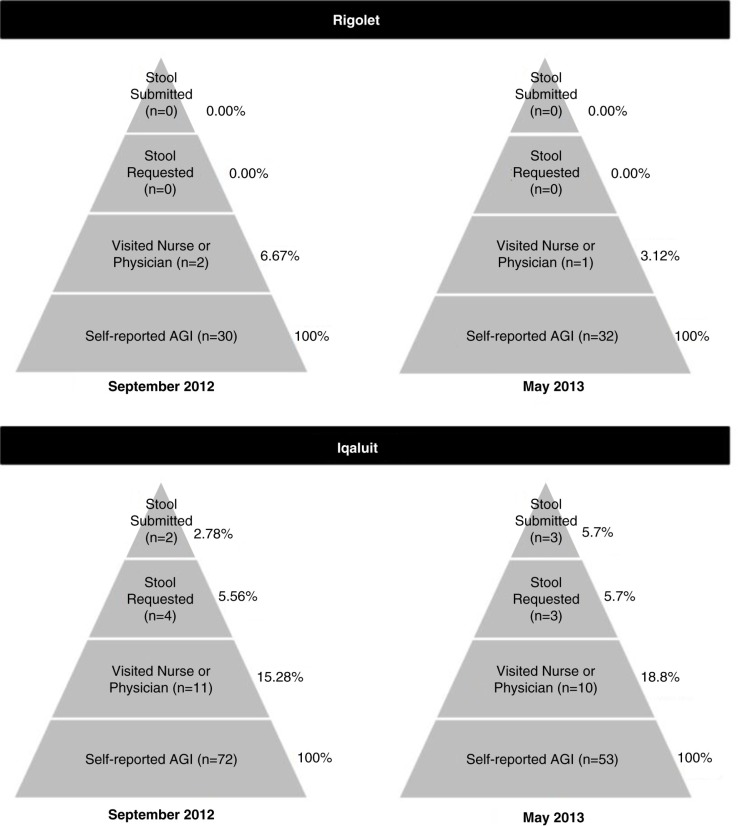
Results: In Rigolet, few AGI cases used healthcare services [4.8% (95% CI=1.5-14.4%)]; in Iqaluit, some cases used healthcare services [16.9% (95% CI=11.2-24.7%)]. Missing traditional activities due to AGI (OR=3.8; 95% CI=1.18-12.4) and taking OTC medication for AGI symptoms (OR=3.8; 95% CI=1.2-15.1) were associated with increased odds of using healthcare services in Iqaluit. In both communities, AGI severity and secondary symptoms (extreme tiredness, headache, muscle pains, chills) were significantly associated with increased odds of taking OTC medication.
Conclusions: While rates of self-reported AGI were higher in Inuit communities compared to non-Inuit communities in Canada, there were lower rates of AGI-related healthcare use in Inuit communities compared to other regions in Canada. As such, the rates of healthcare use for a given disease can differ between Inuit and non-Inuit communities, and caution should be exercised in making comparisons between Inuit and non-Inuit health outcomes based solely on clinic records and healthcare use.
Keywords: Aboriginal health; Indigenous health; Inuit health; Nunatsiavut; Nunavut; gastrointestinal illness; healthcare utilization.
Figures
Similar articles
-
The hidden costs: Identification of indirect costs associated with acute gastrointestinal illness in an Inuit community.PLoS One. 2018 May 16;13(5):e0196990. doi: 10.1371/journal.pone.0196990. eCollection 2018. PLoS One. 2018. PMID: 29768456 Free PMC article.
-
Acute gastrointestinal illness in two Inuit communities: burden of illness in Rigolet and Iqaluit, Canada.Epidemiol Infect. 2015 Oct;143(14):3048-63. doi: 10.1017/S0950268814003744. Epub 2015 Feb 20. Epidemiol Infect. 2015. PMID: 25697261 Free PMC article.
-
Lived experience of acute gastrointestinal illness in Rigolet, Nunatsiavut: "just suffer through it".Soc Sci Med. 2015 Feb;126:86-98. doi: 10.1016/j.socscimed.2014.12.011. Epub 2014 Dec 8. Soc Sci Med. 2015. PMID: 25528558
-
HIV/AIDS Risk and Prevention Issues Among Inuit Living in Nunavut Territory of Canada.In Vivo. 2016 11-12;30(6):905-916. doi: 10.21873/invivo.11012. In Vivo. 2016. PMID: 27815479 Review.
-
Wastewater treatment and public health in Nunavut: a microbial risk assessment framework for the Canadian Arctic.Environ Sci Pollut Res Int. 2018 Nov;25(33):32860-32872. doi: 10.1007/s11356-017-8566-8. Epub 2017 Feb 21. Environ Sci Pollut Res Int. 2018. PMID: 28224339 Review.
Cited by
-
Place, displacement, and health-seeking behaviour among the Ugandan Batwa: A qualitative study.PLOS Glob Public Health. 2024 Jun 12;4(6):e0003321. doi: 10.1371/journal.pgph.0003321. eCollection 2024. PLOS Glob Public Health. 2024. PMID: 38865306 Free PMC article.
-
Inuit Country Food and Health during Pregnancy and Early Childhood in the Circumpolar North: A Scoping Review.Int J Environ Res Public Health. 2021 Mar 5;18(5):2625. doi: 10.3390/ijerph18052625. Int J Environ Res Public Health. 2021. PMID: 33807905 Free PMC article.
-
The need for community-led, integrated and innovative monitoring programmes when responding to the health impacts of climate change.Int J Circumpolar Health. 2019 Jan-Dec;78(2):1517581. doi: 10.1080/22423982.2018.1517581. Int J Circumpolar Health. 2019. PMID: 31066653 Free PMC article.
-
The hidden costs: Identification of indirect costs associated with acute gastrointestinal illness in an Inuit community.PLoS One. 2018 May 16;13(5):e0196990. doi: 10.1371/journal.pone.0196990. eCollection 2018. PLoS One. 2018. PMID: 29768456 Free PMC article.
-
Promoting Inuit health through a participatory whiteboard video.Can J Public Health. 2020 Feb;111(1):50-59. doi: 10.17269/s41997-019-00189-1. Epub 2019 Apr 25. Can J Public Health. 2020. PMID: 31025298 Free PMC article.
References
-
- King M, Smith A, Gracey M. Indigenous health part 2: the underlying causes of the health gap. Lancet. 2009;374:76–85. - PubMed
-
- Marrone S. Understanding barriers to health care: a review of disparities in health care. Int J Circumpolar Health. 2007;66:188–98. - PubMed
-
- Tjepkema M. The Health of the off-reserve aboriginal population. Stat Can. 2002;13:1–17.
-
- Scallan E, Jones TF, Cronquist A, Thomas S, Frenzen P, Hoefer D, et al. Factors associated with seeking medical care and submitting a stool sample in estimating the burden of foodborne illness. Foodborne Pathog Dis. 2006;3:432–8. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials