

High resolution MRI for preoperative work-up of neonates with an anorectal malformation: a direct comparison with distal pressure colostography/fistulography
- PMID: 26002129
- PMCID: PMC4636514
- DOI: 10.1007/s00330-015-3786-0
High resolution MRI for preoperative work-up of neonates with an anorectal malformation: a direct comparison with distal pressure colostography/fistulography
Abstract
Objective: To compare MRI and colostography/fistulography in neonates with anorectal malformations (ARM), using surgery as reference standard.
Methods: Thirty-three neonates (22 boys) with ARM were included. All patients underwent both preoperative high-resolution MRI (without sedation or contrast instillation) and colostography/fistulography. The Krickenbeck classification was used to classify anorectal malformations, and the level of the rectal ending in relation to the levator muscle was evaluated.
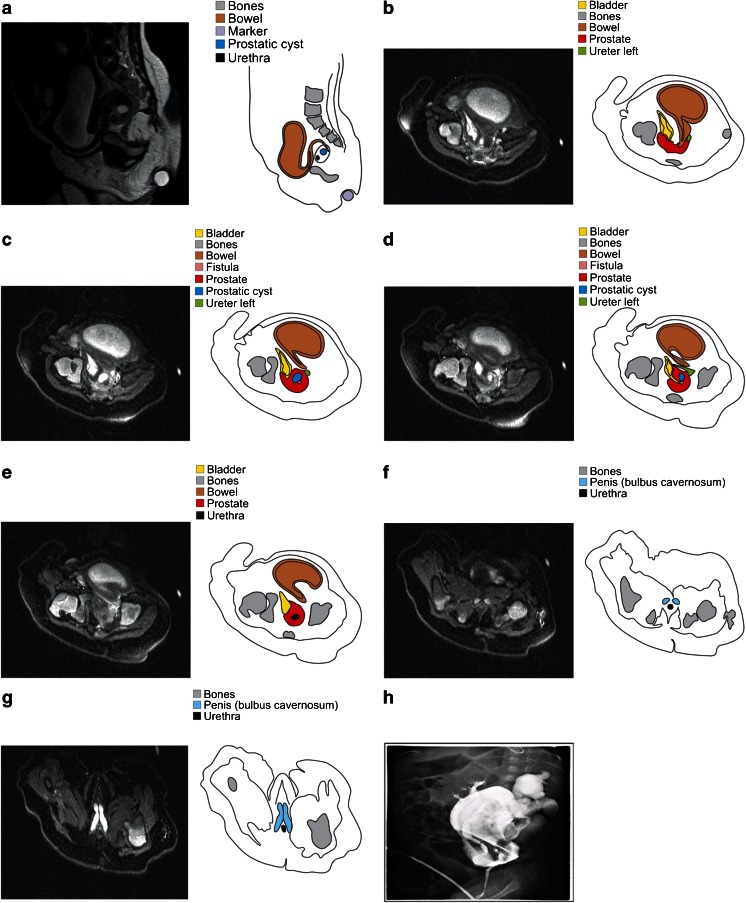
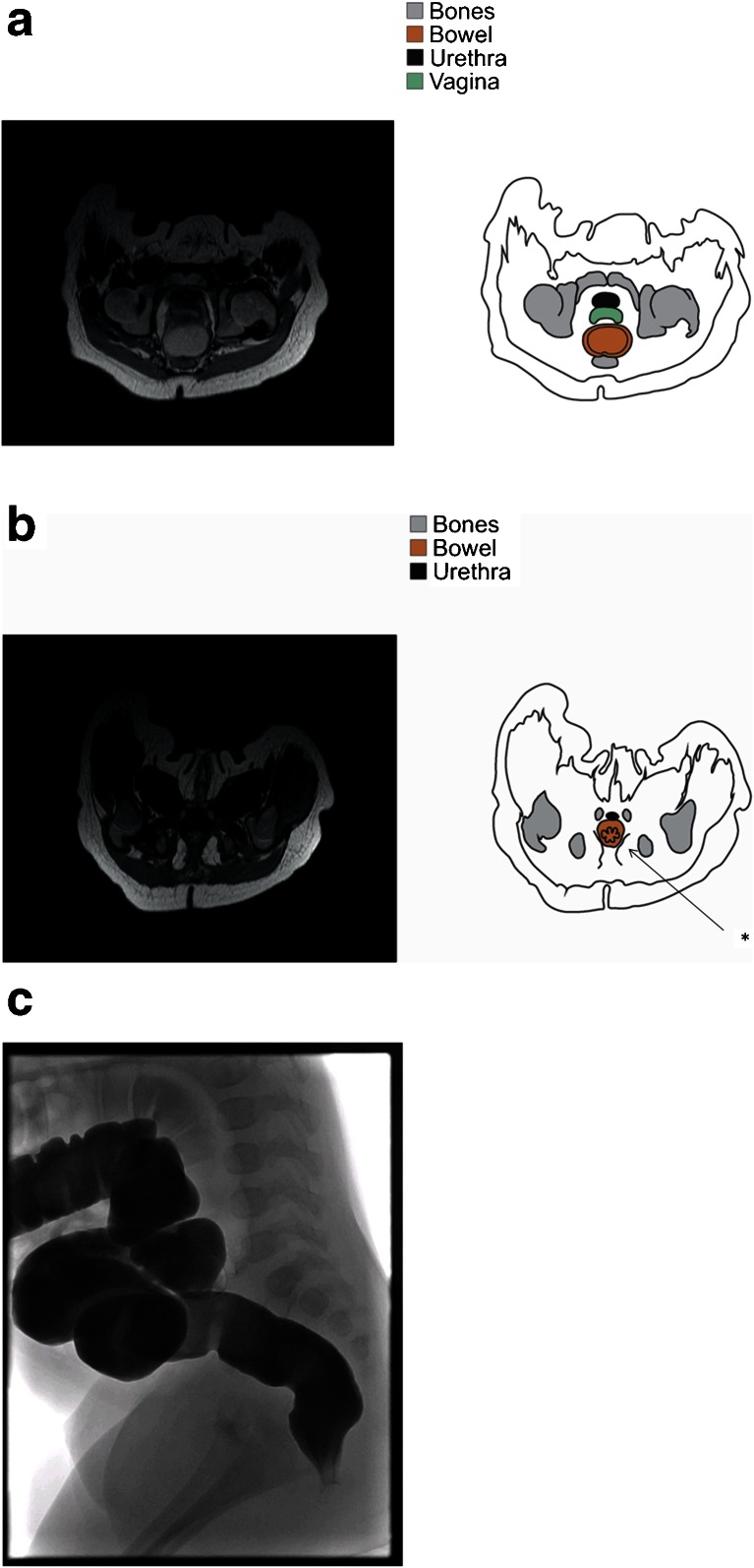
Results: Subjects included nine patients with a bulbar recto-urethral fistula, six with a prostatic recto-urethral fistula, five with a vestibular fistula, five with a cloacal malformation, four without fistula, one with a H-type fistula, one with anal stenosis, one with a rectoperineal fistula and one with a bladderneck fistula. MRI and colostography/fistulography predicted anatomy in 88 % (29/33) and 61 % (20/33) of cases, respectively (p = 0.012). The distal end of the rectal pouch was correctly predicted in 88 % (29/33) and 67 % (22/33) of cases, respectively (p = 0.065). The length of the common channel in cloacal malformation was predicted with MRI in all (100 %, 5/5) and in 80 % of cases (4/5) with colostography/fistulography. Two bowel perforations occurred during colostography/fistulography.
Conclusions: MRI provides the most accurate evaluation of ARM and should be considered a serious alternative to colostography/fistulography during preoperative work-up.
Key points: • High-resolution MRI is feasible without the use of sedation or anaesthesia. • MRI is more accurate than colostography/fistulography in visualising the type of ARM. • MRI is as reliable as colostography/fistulography in predicting the level of the rectal pouch. • Colostography/fistulography can be complicated by bowel perforation.
Keywords: Anorectal malformation; Colostography; Fistulography; MRI; Neonates.
Figures
Similar articles
-
Voiding Cystourethrography in the Diagnosis of Anorectal Malformations.Eur J Pediatr Surg. 2016 Dec;26(6):494-499. doi: 10.1055/s-0035-1570102. Epub 2016 Jan 11. Eur J Pediatr Surg. 2016. PMID: 26752614
-
Comparative effectiveness of imaging modalities for preoperative assessment of anorectal malformation in the pediatric population.J Pediatr Surg. 2019 Dec;54(12):2550-2553. doi: 10.1016/j.jpedsurg.2019.08.037. Epub 2019 Aug 30. J Pediatr Surg. 2019. PMID: 31495505
-
Abnormalities in "low" anorectal malformations (ARMs) and functional results resecting the distal 3 cm.J Pediatr Surg. 2013 Jun;48(6):1294-300. doi: 10.1016/j.jpedsurg.2013.03.026. J Pediatr Surg. 2013. PMID: 23845621
-
[Congenital recto-vaginal fistula associated with a normal anus (type H fistula) and rectal atresia in a patient. Report of a case and a brief revision of the literature].Invest Clin. 2015 Sep;56(3):301-7. Invest Clin. 2015. PMID: 26710545 Review. Spanish.
-
Laparoscopic approach in the management of anorectal malformations.Pediatr Surg Int. 2015 May;31(5):431-7. doi: 10.1007/s00383-015-3687-y. Epub 2015 Mar 1. Pediatr Surg Int. 2015. PMID: 25725614 Review.
Cited by
-
Normal anorectal musculatures and changes in anorectal malformation.Pediatr Surg Int. 2020 Jan;36(1):103-111. doi: 10.1007/s00383-019-04583-1. Epub 2019 Oct 4. Pediatr Surg Int. 2020. PMID: 31586234
-
Ultrasound imaging of the anorectal malformation during the neonatal period: a comprehensive review.Jpn J Radiol. 2018 Oct;36(10):581-591. doi: 10.1007/s11604-018-0767-7. Epub 2018 Aug 17. Jpn J Radiol. 2018. PMID: 30120703 Review.
-
Anorectal malformations.Nat Rev Dis Primers. 2024 Nov 21;10(1):88. doi: 10.1038/s41572-024-00574-2. Nat Rev Dis Primers. 2024. PMID: 39572572 Review.
-
[Gastrointestinal Emergencies in Neonates: What We Should Know].Taehan Yongsang Uihakhoe Chi. 2020 Jul;81(4):770-793. doi: 10.3348/jksr.2020.81.4.770. Epub 2020 Jul 30. Taehan Yongsang Uihakhoe Chi. 2020. PMID: 36238170 Free PMC article. Review. Korean.
-
Anorectal malformation with long perineal fistula: one of a special type.Sci Rep. 2021 Jan 18;11(1):1706. doi: 10.1038/s41598-021-81056-3. Sci Rep. 2021. PMID: 33462249 Free PMC article.
References
-
- Pena A. Posterior sagittal approach for the correction of anorectal malformations. Adv Surg. 1986;19:69–100. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
