

Soft tissue and wound management of blast injuries
- PMID: 26002232
- PMCID: PMC4596198
- DOI: 10.1007/s12178-015-9275-x
Soft tissue and wound management of blast injuries
Abstract
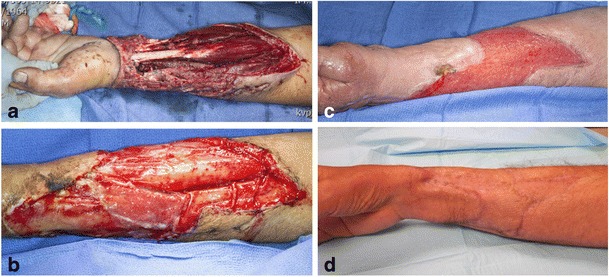
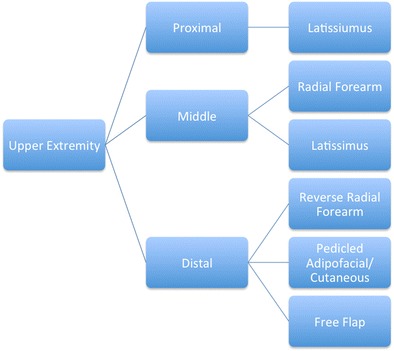
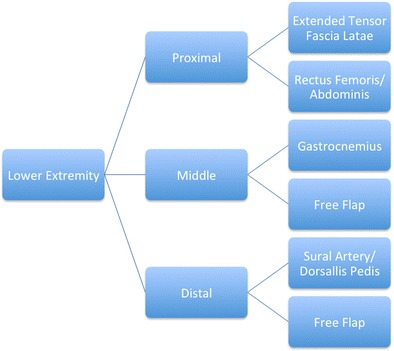
The management of blast-related soft tissue wounds requires a comprehensive surgical approach that acknowledges extensive zones of injury and the likelihood of massive contamination. The experiences of military surgeons during the last decade of war have significantly enhanced current understandings of the optimal means of mitigating infectious complications, the timing of soft tissue coverage attempts, and the reconstructive options available for definitive wound management. Early administration of antibiotics in the setting of soft tissue wounds and associated open fractures is the single most important aspect of open fracture care. Both civilian and military reports have elucidated the incidence of invasive fungal infection in the setting of high-energy injuries with significant wound burdens, and novel treatment protocols have emerged. The type of reconstruction is predicated upon the zone of injury and location of the soft tissue defect. Multiple reports of military cohorts have suggested the equivalency of various techniques and types of soft tissue coverage. Longer-term follow-up will inform future perspectives on the durability of these surgical approaches.
Figures
Similar articles
-
Wartime Soft Tissue Coverage Techniques for the Deployed Surgeon.Mil Med. 2018 Sep 1;183(9-10):e247-e254. doi: 10.1093/milmed/usy022. Mil Med. 2018. PMID: 29590411
-
A staged protocol for soft tissue management in the treatment of complex pilon fractures.J Orthop Trauma. 2004 Sep;18(8 Suppl):S32-8. doi: 10.1097/00005131-200409001-00005. J Orthop Trauma. 2004. PMID: 15472563
-
A staged protocol for soft tissue management in the treatment of complex pilon fractures.J Orthop Trauma. 1999 Feb;13(2):78-84. doi: 10.1097/00005131-199902000-00002. J Orthop Trauma. 1999. PMID: 10052780
-
Changing paradigms in lower extremity reconstruction in war-related injuries.Mil Med Res. 2016 Mar 31;3:9. doi: 10.1186/s40779-016-0080-7. eCollection 2016. Mil Med Res. 2016. PMID: 27042328 Free PMC article. Review.
-
Approach to Complex Lower Extremity Reconstruction.Semin Plast Surg. 2022 Nov 16;36(4):233-242. doi: 10.1055/s-0042-1758205. eCollection 2022 Nov. Semin Plast Surg. 2022. PMID: 36561427 Free PMC article. Review.
Cited by
-
Cell-mediated remodeling of biomimetic encapsulating hydrogels triggered by adipogenic differentiation of adipose stem cells.J Tissue Eng. 2016 Sep 23;7:2041731416670482. doi: 10.1177/2041731416670482. eCollection 2016 Jan-Dec. J Tissue Eng. 2016. PMID: 27733898 Free PMC article.
-
Molecular Detection of Filamentous Fungi in Formalin-Fixed Paraffin-Embedded Specimens in Invasive Fungal Wound Infections Is Feasible with High Specificity.J Clin Microbiol. 2019 Dec 23;58(1):e01259-19. doi: 10.1128/JCM.01259-19. Print 2019 Dec 23. J Clin Microbiol. 2019. PMID: 31619528 Free PMC article.
-
Epidemiology of Injuries Sustained by Civilians and Local Combatants in Contemporary Armed Conflict: An Appeal for a Shared Trauma Registry Among Humanitarian Actors.World J Surg. 2020 Jun;44(6):1863-1873. doi: 10.1007/s00268-020-05428-y. World J Surg. 2020. PMID: 32100067 Free PMC article. Review.
-
[Treatment strategies for mass casualty incidents and terrorist attacks in trauma and vascular surgery : Presentation of a treatment concept].Chirurg. 2017 Oct;88(10):856-862. doi: 10.1007/s00104-017-0490-4. Chirurg. 2017. PMID: 28801785 Review. German.
-
Designed Antimicrobial Peptides Against Trauma-Related Cutaneous Invasive Fungal Wound Infections.J Fungi (Basel). 2020 Sep 22;6(3):184. doi: 10.3390/jof6030184. J Fungi (Basel). 2020. PMID: 32971819 Free PMC article.
References
-
- Emergency War Surgery, Fourth Revision. U.S. Department of Defense, U.S. Army, Office of the Surgeon General, 2014. Print.
-
- Centers for Disease Control. Explosions and blast injuries: a primer for clinicians. Centers for Disease Control; 2007, Atlanta, GA.
-
- Taxonomy of injuries from explosive devices. Medical Research for Prevention, Mitigation, and Treatment of Blast Injuries. Washington, DC: Department of Defense. Enclosure, 2, 9, July 5, 2006.
-
- Fleming M, Waterman S, Dunne J, D’Alleyrand JC, Andersen RC. Dismounted complex blast injuries: patterns of injuries and resource utilization associated with the multiple extremity amputee. J Surg Orthop Adv. 2012;212(1):32–7. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
