

False positive and false negative diagnoses of prostate cancer at multi-parametric prostate MRI in active surveillance
- PMID: 26002487
- PMCID: PMC4519810
- DOI: 10.1007/s13244-015-0411-3
False positive and false negative diagnoses of prostate cancer at multi-parametric prostate MRI in active surveillance
Abstract
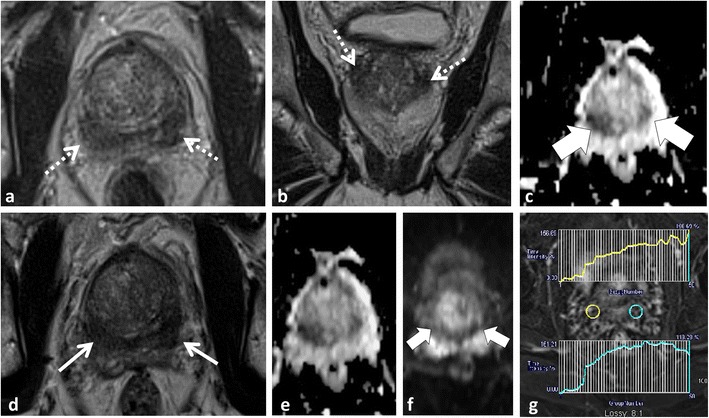
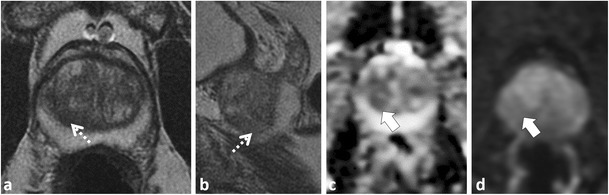
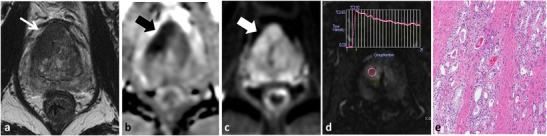
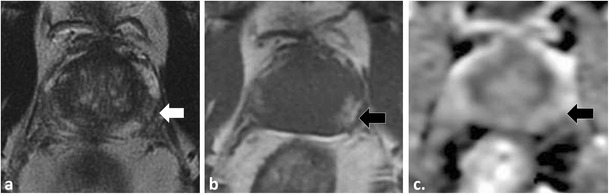
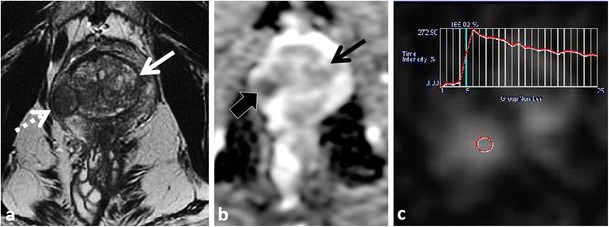
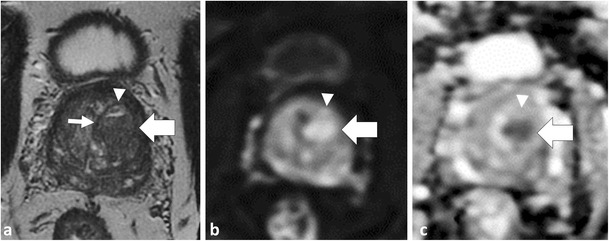
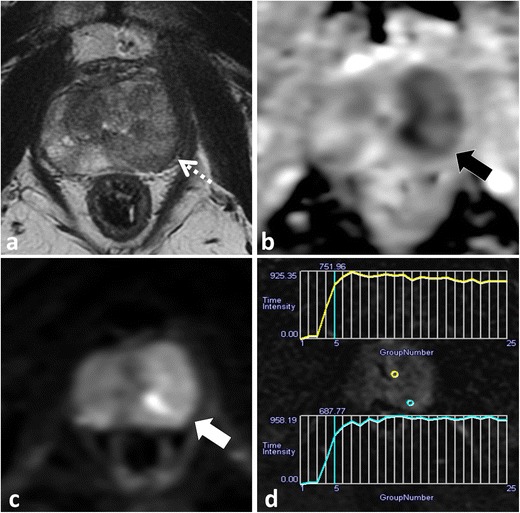
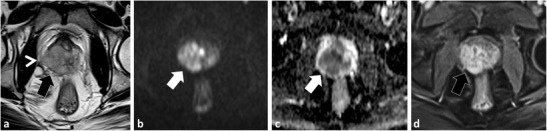
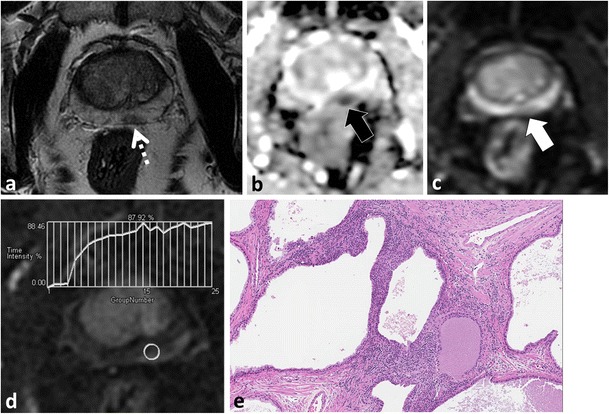
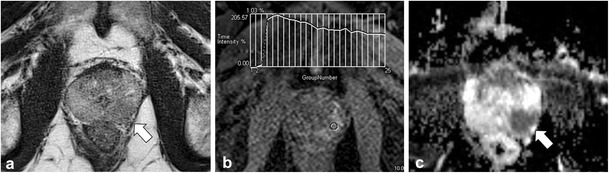
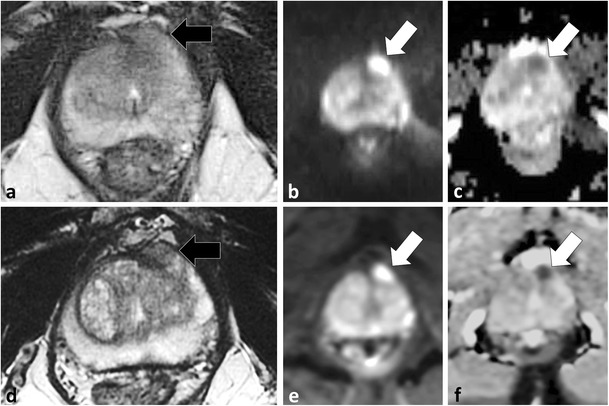
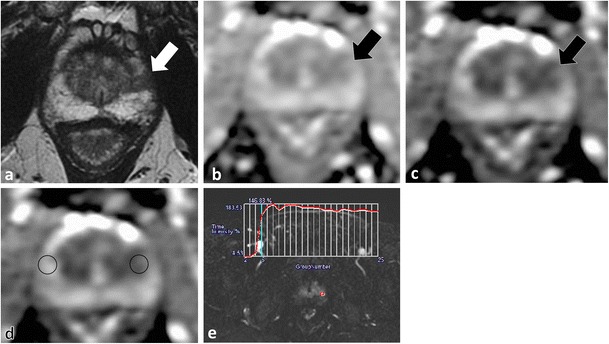
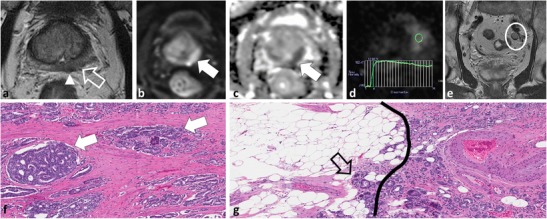
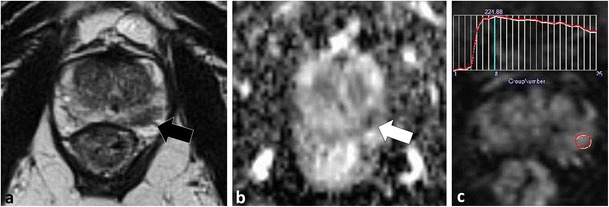
MP-MRI is a critical component in active surveillance (AS) of prostate cancer (PCa) because of a high negative predictive value for clinically significant tumours. This review illustrates pitfalls of MP-MRI and how to recognise and avoid them. The anterior fibromuscular stroma and central zone are low signal on T2W-MRI/apparent diffusion coefficient (ADC), resembling PCa. Location, progressive enhancement and low signal on b ≥1000 mm²/s echo-planar images (EPI) are differentiating features. BPH can mimic PCa. Glandular BPH shows increased T2W/ADC signal, cystic change and progressive enhancement; however, stromal BPH resembles transition zone (TZ) PCa. A rounded morphology, low T2 signal capsule and posterior/superior location favour stromal BPH. Acute/chronic prostatitis mimics PCa at MP-MRI, with differentiation mainly on clinical grounds. Visual analysis of diffusion-weighted MRI must include EPI and appropriate windowing of ADC. Quantitative ADC analysis is limited by lack of standardization; the ADC ratio and ADC histogram analysis are alternatives to mean values. DCE lacks standardisation and has limited utility in the TZ, where T2W/DWI are favoured. Targeted TRUS-guided biopsies of MR-detected lesions are challenging. Lesions detected on MP-MRI may not be perfectly targeted with TRUS and this must be considered when faced with a suspicious lesion on MP-MRI and a negative targeted TRUS biopsy histopathological result.
Keypoints: • Multi-parametric MRI plays a critical role in prostate cancer active surveillance. • Low T2W signal intensity structures appear dark on ADC, potentially simulating cancer. • Stromal BPH mimics cancer at DWI and DCE. • Long b value trace EPI should be reviewed • Targeted biopsy of MR-detected lesions using TRUS guidance may be challenging.
Figures


Similar articles
-
Multiparametric MRI in detection and staging of prostate cancer.Dan Med J. 2017 Feb;64(2):B5327. Dan Med J. 2017. PMID: 28157066 Review.
-
Differentiation of prostate cancer lesions in the Transition Zone by diffusion-weighted MRI.Eur J Radiol Open. 2017 Sep 29;4:123-128. doi: 10.1016/j.ejro.2017.08.003. eCollection 2017. Eur J Radiol Open. 2017. PMID: 29034282 Free PMC article.
-
Revisiting quantitative multi-parametric MRI of benign prostatic hyperplasia and its differentiation from transition zone cancer.Abdom Radiol (NY). 2019 Jun;44(6):2233-2243. doi: 10.1007/s00261-019-01936-1. Abdom Radiol (NY). 2019. PMID: 30955071
-
Amide Proton Transfer Could Provide More Accurate Lesion Characterization in the Transition Zone of the Prostate.J Magn Reson Imaging. 2022 Nov;56(5):1311-1319. doi: 10.1002/jmri.28204. Epub 2022 Apr 16. J Magn Reson Imaging. 2022. PMID: 35429190
-
Multiparametric MRI of the anterior prostate gland: clinical-radiological-histopathological correlation.Clin Radiol. 2016 May;71(5):405-17. doi: 10.1016/j.crad.2016.01.002. Epub 2016 Feb 14. Clin Radiol. 2016. PMID: 26888762 Review.
Cited by
-
Diffusion kurtosis imaging and standard diffusion imaging in the magnetic resonance imaging assessment of prostate cancer.Gland Surg. 2023 Dec 26;12(12):1806-1822. doi: 10.21037/gs-23-53. Epub 2023 Dec 22. Gland Surg. 2023. PMID: 38229839 Free PMC article. Review.
-
Synthetic correlated diffusion imaging hyperintensity delineates clinically significant prostate cancer.Sci Rep. 2022 Mar 1;12(1):3376. doi: 10.1038/s41598-022-06872-7. Sci Rep. 2022. PMID: 35232991 Free PMC article.
-
False-positive magnetic resonance imaging prostate cancer correlates and clinical implications.Urol Ann. 2023 Jan-Mar;15(1):54-59. doi: 10.4103/ua.ua_22_22. Epub 2022 Nov 8. Urol Ann. 2023. PMID: 37006206 Free PMC article.
-
Multiparametric [11C]Acetate positron emission tomography-magnetic resonance imaging in the assessment and staging of prostate cancer.PLoS One. 2017 Jul 18;12(7):e0180790. doi: 10.1371/journal.pone.0180790. eCollection 2017. PLoS One. 2017. PMID: 28719629 Free PMC article.
-
Discrepancy between Multiparametric Magnetic Resonance Imaging and 68Ga Prostate-Specific Membrane Antigen Positron Emission Tomography: A Simultaneous Acquired Positron Emission Tomography-Magnetic Resonance Imaging Case.Indian J Nucl Med. 2021 Jan-Mar;36(1):50-52. doi: 10.4103/ijnm.IJNM_115_20. Epub 2021 Mar 4. Indian J Nucl Med. 2021. PMID: 34040297 Free PMC article.
References
-
- National Comprehensive Cancer Network NCCN (2012) Clinical practice guidelines in oncology: prostate cancer. Fort Washington, PA. Available via http://www.nccn.com/files/cancer-guidelines/prostate/index.html#/1. Accessed Sept. 13 2013
-
- Prostate Cancer Canada (2014) Prostate cancer Canada network. Toronto, ON Canada. Available via http://prostatecancer.ca. Accessed Sept. 2014
-
- European Association of Urology (EAU) (2012) Guidelines on prostate cancer. Arnhem, The Netherlands. Available via http://www.uroweb.org/gls/pdf/08%20Prostate%20Cancer_LR%20March%2013th%2...
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
