

Lenalidomide augments actin remodeling and lowers NK-cell activation thresholds
- PMID: 26002964
- PMCID: PMC4551357
- DOI: 10.1182/blood-2015-01-625004
Lenalidomide augments actin remodeling and lowers NK-cell activation thresholds
Abstract
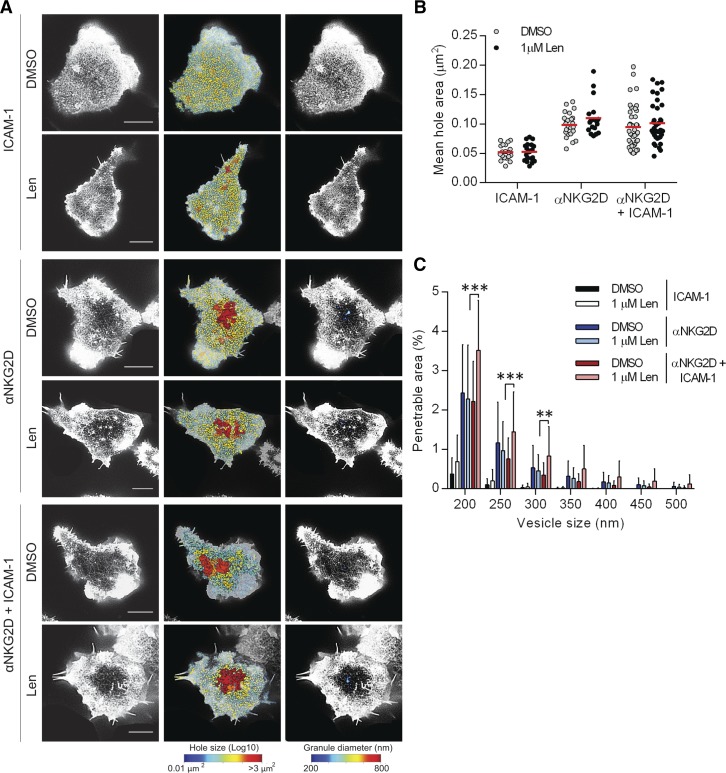
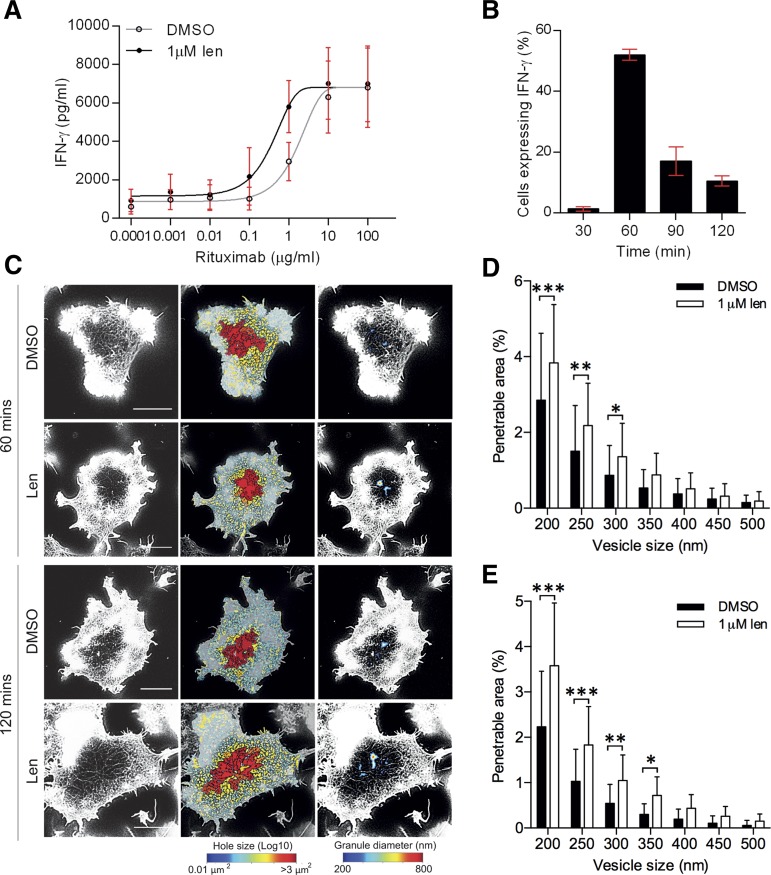
As multiple myeloma (MM) progresses, natural killer (NK)-cell responses decline against malignant plasma cells. The immunomodulatory drug lenalidomide is widely used for treatment of MM but its influence on NK-cell biology is unclear. Here, we report that lenalidomide lowers the threshold for NK-cell activation, causing a 66% decrease in the 50% effective concentration (EC50) for activation through CD16, and a 38% decrease in EC50 for NK group 2 member D (NKG2D)-mediated activation, allowing NK cells to respond to lower doses of ligand. In addition, lenalidomide augments NK-cell responses, causing a twofold increase in the proportion of primary NK cells producing interferon-γ (IFN-γ), and a 20-fold increase in the amount of IFN-γ produced per cell. Importantly, lenalidomide did not trigger IFN-γ production in unstimulated NK cells. Thus, lenalidomide enhances the NK-cell arm of the immune response, without activating NK cells inappropriately. Of particular clinical importance, lenalidomide also allowed NK cells to be activated by lower doses of rituximab, an anti-CD20 monoclonal antibody (mAb) widely used to treat B-cell malignancies. This supports combined use of lenalidomide and rituximab in a clinical setting. Finally, superresolution microscopy revealed that lenalidomide increased the periodicity of cortical actin at immune synapses, resulting in an increase in the area of the actin mesh predicted to be penetrable to vesicles containing IFN-γ. NK cells from MM patients also responded to lenalidomide in this way. This indicates that nanometer-scale rearrangements in cortical actin, a recently discovered step in immune synapse assembly, are a potential new target for therapeutic compounds.
© 2015 by The American Society of Hematology.
Figures





Similar articles
-
Lenalidomide enhances antibody-dependent cellular cytotoxicity of solid tumor cells in vitro: influence of host immune and tumor markers.Cancer Immunol Immunother. 2011 Jan;60(1):61-73. doi: 10.1007/s00262-010-0919-9. Epub 2010 Sep 17. Cancer Immunol Immunother. 2011. PMID: 20848094 Free PMC article.
-
Remodelling of cortical actin where lytic granules dock at natural killer cell immune synapses revealed by super-resolution microscopy.PLoS Biol. 2011 Sep;9(9):e1001152. doi: 10.1371/journal.pbio.1001152. Epub 2011 Sep 13. PLoS Biol. 2011. PMID: 21931537 Free PMC article.
-
lenalidomide enhances natural killer cell and monocyte-mediated antibody-dependent cellular cytotoxicity of rituximab-treated CD20+ tumor cells.Clin Cancer Res. 2008 Jul 15;14(14):4650-7. doi: 10.1158/1078-0432.CCR-07-4405. Clin Cancer Res. 2008. PMID: 18628480
-
Mechanisms of NK Cell Activation and Clinical Activity of the Therapeutic SLAMF7 Antibody, Elotuzumab in Multiple Myeloma.Front Immunol. 2018 Nov 5;9:2551. doi: 10.3389/fimmu.2018.02551. eCollection 2018. Front Immunol. 2018. PMID: 30455698 Free PMC article. Review.
-
Properties of thalidomide and its analogues: implications for anticancer therapy.AAPS J. 2005 Mar 22;7(1):E14-9. doi: 10.1208/aapsj070103. AAPS J. 2005. PMID: 16146335 Free PMC article. Review.
Cited by
-
The homeobox transcription factor MEIS2 is a regulator of cancer cell survival and IMiDs activity in Multiple Myeloma: modulation by Bromodomain and Extra-Terminal (BET) protein inhibitors.Cell Death Dis. 2019 Apr 11;10(4):324. doi: 10.1038/s41419-019-1562-9. Cell Death Dis. 2019. PMID: 30975979 Free PMC article.
-
Mechanisms of Action of the New Antibodies in Use in Multiple Myeloma.Front Oncol. 2021 Jul 8;11:684561. doi: 10.3389/fonc.2021.684561. eCollection 2021. Front Oncol. 2021. PMID: 34307150 Free PMC article. Review.
-
A comprehensive review of lenalidomide in B-cell non-Hodgkin lymphoma.Ther Adv Hematol. 2016 Aug;7(4):209-21. doi: 10.1177/2040620716652861. Epub 2016 Jul 1. Ther Adv Hematol. 2016. PMID: 27493711 Free PMC article. Review.
-
AUGMENT: A Phase III Study of Lenalidomide Plus Rituximab Versus Placebo Plus Rituximab in Relapsed or Refractory Indolent Lymphoma.J Clin Oncol. 2019 May 10;37(14):1188-1199. doi: 10.1200/JCO.19.00010. Epub 2019 Mar 21. J Clin Oncol. 2019. PMID: 30897038 Free PMC article. Clinical Trial.
-
Role of the tumor microenvironment in mature B-cell lymphoid malignancies.Haematologica. 2016 May;101(5):531-40. doi: 10.3324/haematol.2015.139493. Haematologica. 2016. PMID: 27132279 Free PMC article. Review.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
