

Emergency Department Crowding and Outcomes After Emergency Department Discharge
- PMID: 26003004
- PMCID: PMC5270644
- DOI: 10.1016/j.annemergmed.2015.04.009
Emergency Department Crowding and Outcomes After Emergency Department Discharge
Abstract
Study objective: We assess whether a panel of emergency department (ED) crowding measures, including 2 reported by the Centers for Medicare & Medicaid Services (CMS), is associated with inpatient admission and death within 7 days of ED discharge.
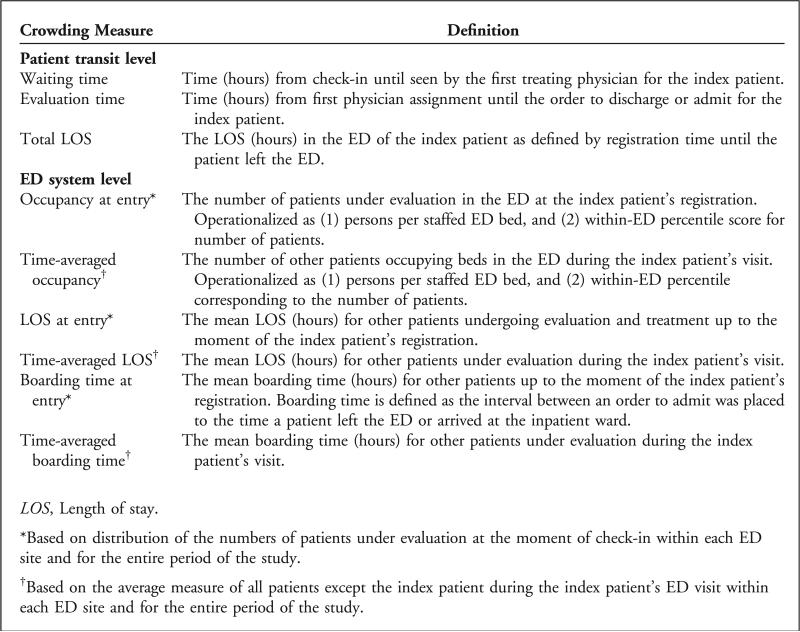
Methods: We conducted a retrospective cohort study of ED discharges, using data from an integrated health system for 2008 to 2010. We assessed patient transit-level (n=3) and ED system-level (n=6) measures of crowding, using multivariable logistic regression models. The outcome measures were inpatient admission or death within 7 days of ED discharge. We defined a clinically important association by assessing the relative risk ratio and 95% confidence interval (CI) difference and also compared risks at the 99th percentile and median value of each measure.
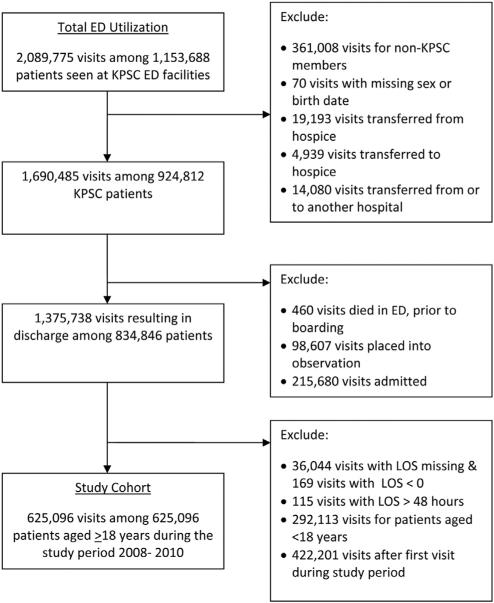
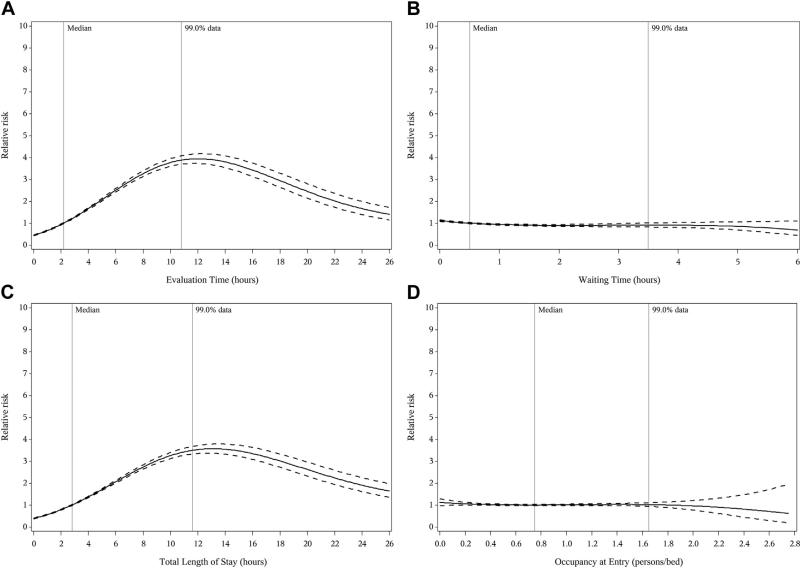
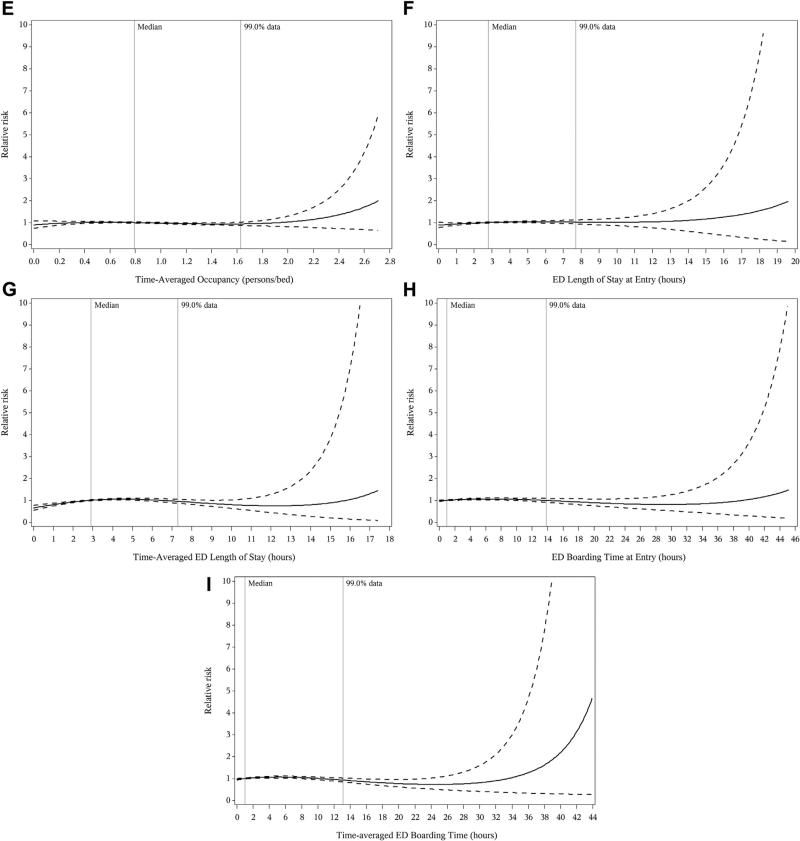
Results: The study cohort contained a total of 625,096 visits to 12 EDs. There were 16,957 (2.7%) admissions and 328 (0.05%) deaths within 7 days. Only 2 measures, both of which were patient transit measures, were associated with the outcome. Compared with a median evaluation time of 2.2 hours, the evaluation time of 10.8 hours (99th percentile) was associated with a relative risk of 3.9 (95% CI 3.7 to 4.1) of an admission. Compared with a median ED length of stay (a CMS measure) of 2.8 hours, the 99th percentile ED length of stay of 11.6 hours was associated with a relative risk of 3.5 (95% CI 3.3 to 3.7) of admission. No system measure of ED crowding was associated with outcomes.
Conclusion: Our findings suggest that ED length of stay is a proxy for unmeasured differences in case mix and challenge the validity of the CMS metric as a safety measure for discharged patients.
Copyright © 2015 American College of Emergency Physicians. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Emergency Care at the Crossroads: Emergency Department Crowding, Payment Reform, and One Potential Future.Ann Emerg Med. 2015 Nov;66(5):493-5. doi: 10.1016/j.annemergmed.2015.05.013. Epub 2015 Jun 6. Ann Emerg Med. 2015. PMID: 26059488 No abstract available.
Similar articles
-
Emergency department crowding predicts admission length-of-stay but not mortality in a large health system.Med Care. 2014 Jul;52(7):602-11. doi: 10.1097/MLR.0000000000000141. Med Care. 2014. PMID: 24926707 Free PMC article.
-
Effect of emergency department crowding on outcomes of admitted patients.Ann Emerg Med. 2013 Jun;61(6):605-611.e6. doi: 10.1016/j.annemergmed.2012.10.026. Epub 2012 Dec 6. Ann Emerg Med. 2013. PMID: 23218508 Free PMC article.
-
Characteristics of ED crowding in the Lazio Region (Italy) and short-term health outcomes.Intern Emerg Med. 2019 Jan;14(1):109-117. doi: 10.1007/s11739-018-1881-3. Epub 2018 May 25. Intern Emerg Med. 2019. PMID: 29802522 Free PMC article.
-
Comparison of methods for measuring crowding and its effects on length of stay in the emergency department.Acad Emerg Med. 2011 Dec;18(12):1269-77. doi: 10.1111/j.1553-2712.2011.01232.x. Acad Emerg Med. 2011. PMID: 22168190 Review.
-
Improving emergency department flow by introducing four interventions simultaneously. A quality improvement project.Int Emerg Nurs. 2024 Sep;76:101499. doi: 10.1016/j.ienj.2024.101499. Epub 2024 Aug 10. Int Emerg Nurs. 2024. PMID: 39128253 Review.
Cited by
-
Length-of-Stay in the Emergency Department and In-Hospital Mortality: A Systematic Review and Meta-Analysis.J Clin Med. 2022 Dec 21;12(1):32. doi: 10.3390/jcm12010032. J Clin Med. 2022. PMID: 36614835 Free PMC article. Review.
-
Challenges, consequences, and lessons for way-outs to emergencies at hospitals: a systematic review study.BMC Emerg Med. 2019 Oct 30;19(1):62. doi: 10.1186/s12873-019-0275-9. BMC Emerg Med. 2019. PMID: 31666023 Free PMC article.
-
Prevalence of crowding, boarding and staffing levels in Swedish emergency departments - a National Cross Sectional Study.BMC Emerg Med. 2020 Jun 18;20(1):50. doi: 10.1186/s12873-020-00342-x. BMC Emerg Med. 2020. PMID: 32552701 Free PMC article.
-
Effects of crowding in the emergency department on the diagnosis and management of suspected acute coronary syndrome using rapid algorithms: an observational study.BMJ Open. 2020 Oct 8;10(10):e041757. doi: 10.1136/bmjopen-2020-041757. BMJ Open. 2020. PMID: 33033102 Free PMC article.
-
The Association between Emergency Department Length of Stay and In-Hospital Mortality in Older Patients Using Machine Learning: An Observational Cohort Study.J Clin Med. 2023 Jul 18;12(14):4750. doi: 10.3390/jcm12144750. J Clin Med. 2023. PMID: 37510865 Free PMC article.
References
-
- Institute of Medicine: Future of Emergency Care: Hospital-Based Emergency Care at the Breaking Point. National Academic Press; Washington, DC: 2006.
-
- Pines JM. Emergency department crowding in California: a silent killer? Ann Emerg Med. 2013;61:612–614. - PubMed
-
- Bernstein S, Aronsky D, Duseja R, et al. The effect of emergency department crowding on clinically oriented outcomes. Acad Emerg Med. 2009;16:1–10. - PubMed
-
- Medicare.gov. [December 6, 2014];Hospital compare measures. Available at: http://www.medicare.gov/hospitalcompare/Data/Measures-Displayed.html.
-
- Pines J, Localio A, Hollander J, et al. The impact of emergency department crowding measures on time to antibiotics for. Ann Emerg Med. 2007;50:510–516. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
