

Preliminary Safety, Pharmacokinetics, and Efficacy of Regorafenib, Cisplatin, and Pemetrexed in Patients With Advanced Nonsquamous Non-Small-Cell Lung Cancers
- PMID: 26003007
- PMCID: PMC4750397
- DOI: 10.1016/j.cllc.2015.04.003
Preliminary Safety, Pharmacokinetics, and Efficacy of Regorafenib, Cisplatin, and Pemetrexed in Patients With Advanced Nonsquamous Non-Small-Cell Lung Cancers
Abstract
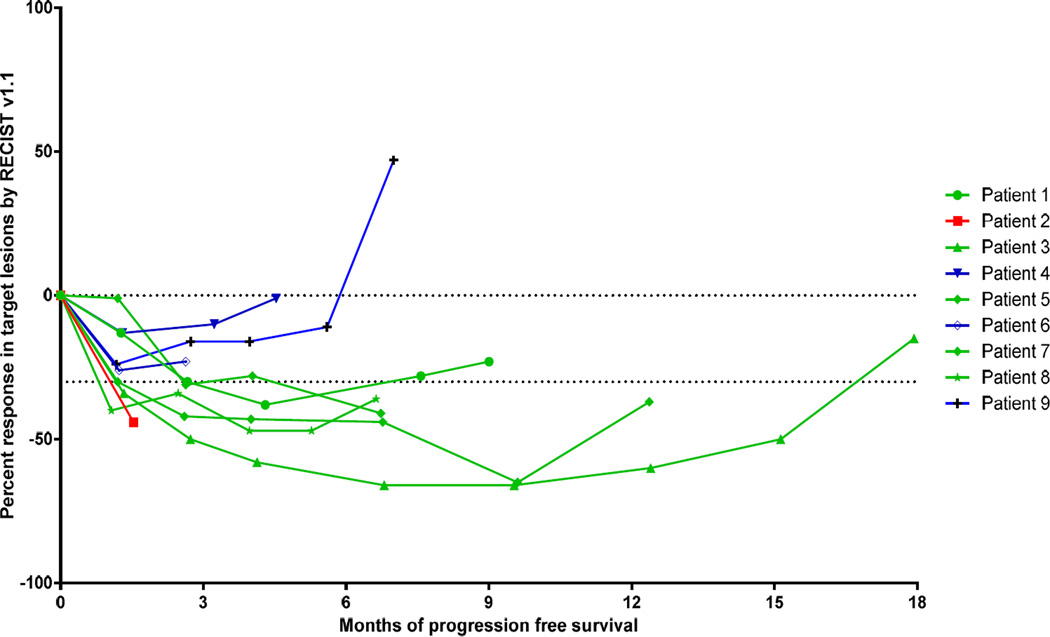
Regorafenib is an oral multitargeted kinase inhibitor with potent antiangiogenic activity. In this phase I trial we evaluated the safety, pharmacokinetics, and efficacy of regorafenib with cisplatin and pemetrexed for patients with advanced nonsquamous non-small-cell lung cancers (nsNSCLCs). Nine patients enrolled before premature termination of the study. Five of 9 (56%) patients had a partial response and the median progression-free survival was 7 months (range, 1.5-15.1 months). Regorafenib had acceptable tolerability and minor pharmacokinetic interactions in combination with standard doses of cisplatin and pemetrexed in patients with advanced nsNSCLCs.
Background: The combination of bevacizumab, an antiangiogenesis agent, with cytotoxic chemotherapy improves survival in patients with advanced nonsquamous non-small-cell lung cancers (nsNSCLCs). Regorafenib is an oral multitargeted kinase inhibitor with potent antiangiogenic activity that is approved for patients with advanced colorectal cancer and gastrointestinal stromal tumors. In this phase I trial we evaluated the safety, pharmacokinetics (PK), and efficacy of regorafenib with cisplatin and pemetrexed for patients with advanced nsNSCLCs.
Patients and methods: Chemotherapy-naive patients with advanced nsNSCLCs were treated with regorafenib 60 mg/d continuously and cisplatin 75 mg/m(2) with pemetrexed 500 mg/m(2) once every 21 days for up to 6 cycles. Thereafter, regorafenib with or without pemetrexed could be continued as maintenance.
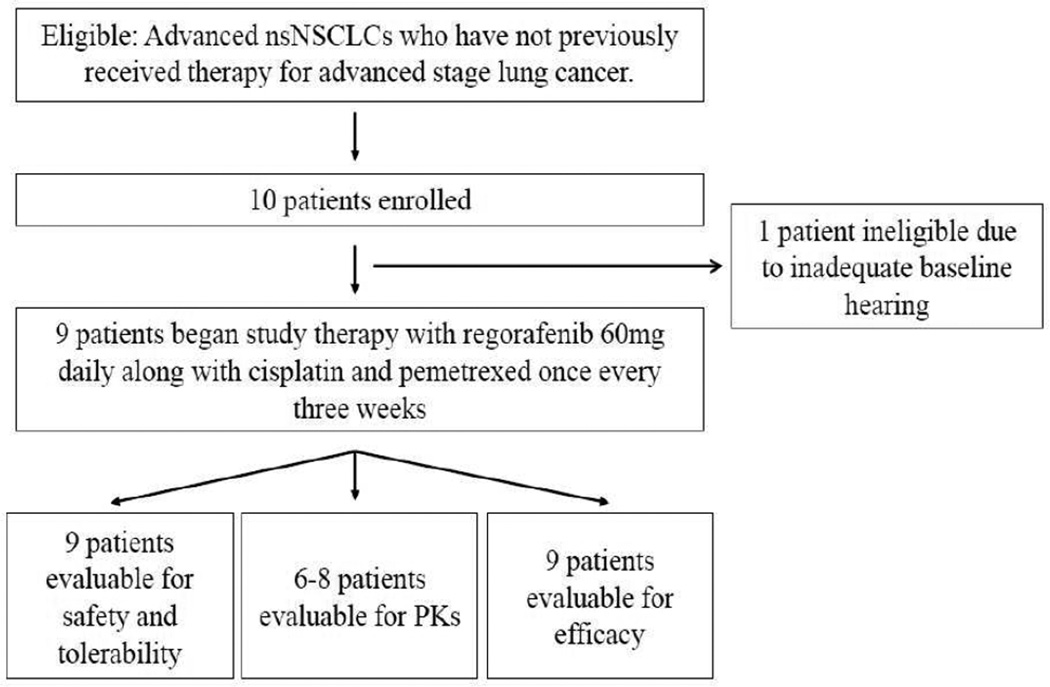
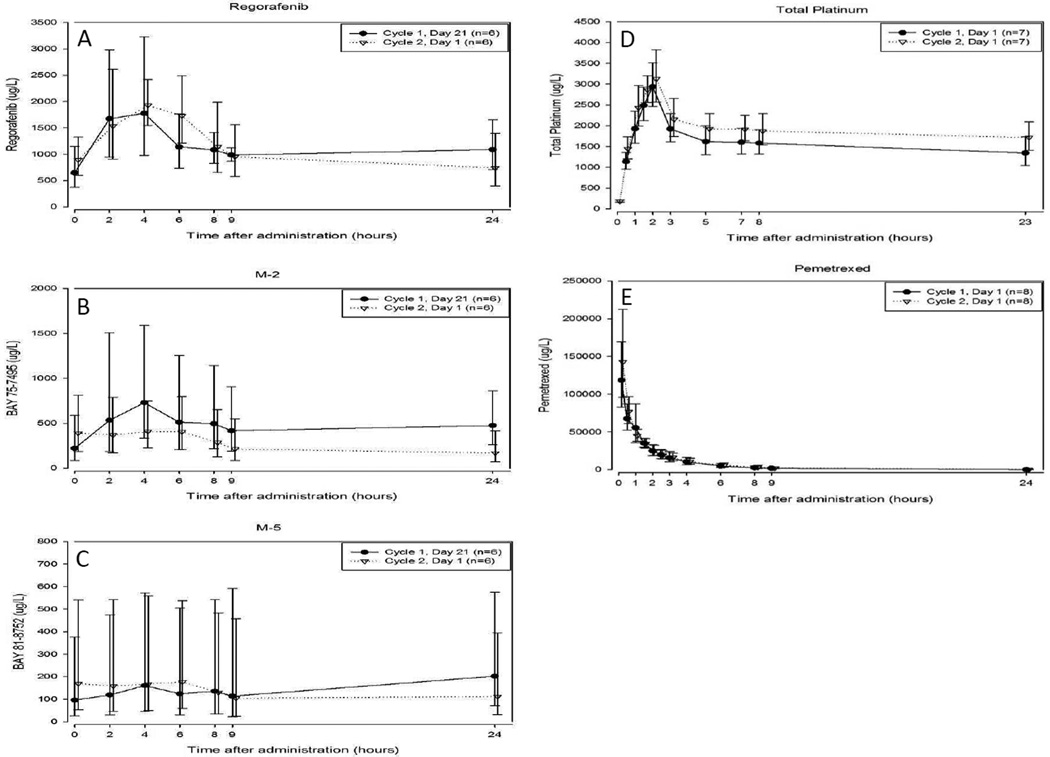
Results: Nine patients enrolled before premature termination of the study because of slow recruitment and a change in the development strategy of regorafenib by the study sponsor. Five patients experienced at least 1 treatment-related Grade 3 adverse event. No Grade 4 or 5 toxicity occurred. Five of 9 (56%) patients had a partial response and the median progression-free survival was 7 months (range, 1.5-15.1 months). Minor PK interactions between regorafenib and chemotherapy were observed.
Conclusion: Regorafenib had acceptable tolerability and minor PK interactions in combination with standard doses of cisplatin and pemetrexed in patients with advanced nsNSCLCs. Encouraging activity was appreciated in chemotherapy-naive patients with advanced nsNSCLCs. However, the small number of patients treated limits conclusions that can be drawn from these results.
Trial registration: ClinicalTrials.gov NCT01187615.
Keywords: Angiogenesis; Chemotherapy; Clinical Trial; NSCLC; Regorafenib.
Copyright © 2015 Elsevier Inc. All rights reserved.
Figures
References
-
- Siegel R, Naishadham D, Jemal A. Cancer Statistics, 2013, CA. A Cancer Journal for Clinicians. 2013;63(1):11–30. - PubMed
-
- Goldstraw P, Crowley J, Chansky K, Giroux DJ, Groome PA, Rami-Porta R, et al. The IASLC lung cancer staging project: Proposals for the revision of he TNM stage groupings in the forthcoming (seventh) edition of the TNM classification of malignant tumours. Journal of Thoracic Oncology. 2007;2(8):706–714. - PubMed
-
- Sandler A, Gray R, Perry MC, Brahmer J, Schiller JH, Dowlati A, et al. Paclitaxel-carboplatin alone or with bevacizumab for non-small-cell lung cancer. The New England Journal of Medicine. 2006;355(24):2542–2550. - PubMed
-
- Wilhelm SM, Dumas J, Adnane L, Lynch M, Carter CA, Schutz G, et al. Regorafenib (BAY 73–4506): a new oral multikinase inhibitor of angiogenic, stromal and oncogenic receptor tyrosine kinases with potent preclinical antitumor activity. International Journal of Cancer Journal. 2011;129(1):245–255. - PubMed
-
- Grothey A, Van Cutsem E, Sobrero A, Siena S, Falcone A, Ychou M, et al. Regorafenib monotherapy for previously treated metastatic colorectal cancer (CORRECT): an international, multicentre, randomised, placebo-controlled, phase 3 trial. Lancet. 2013;381(9863):303–312. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
