

Assessment of mucosal healing in inflammatory bowel disease: review
- PMID: 26005012
- PMCID: PMC6709676
- DOI: 10.1016/j.gie.2015.03.1974
Assessment of mucosal healing in inflammatory bowel disease: review
Abstract
Background and aims: Mucosal healing is an important treatment end-point in inflammatory bowel disease, and achieving mucosal healing has been demonstrated to improve disease-related outcomes. Considerable uncertainty exists, however, regarding the optimal approach for the assessment of mucosal healing.
Aims: To compare currently available diagnostic tools for the assessment of mucosal healing and outline the ideal approach to integrating these tools into clinical trials and clinical practice.
Methods: Review article.
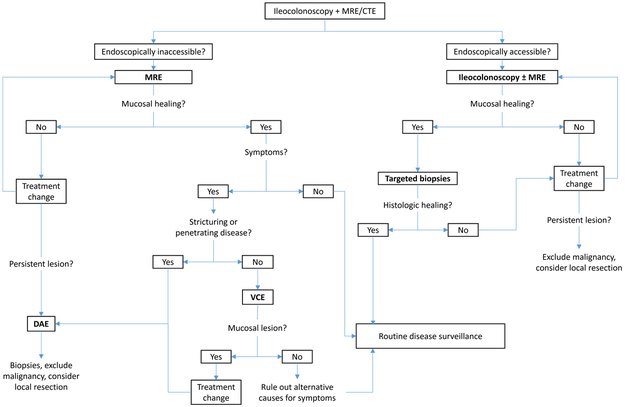
Results: Endoscopy represents the criterion standard for the assessment of mucosal healing, and frequent endoscopic assessment is associated with a higher rate of achieving mucosal healing. The use of mucosal biopsy allows for the identification of persistent histologic disease activity, but the incremental clinical benefit of achieving histologic healing is yet to be determined. Magnetic resonance enterography has a high sensitivity for ulcer healing in endoscopically inaccessible disease activity. However, the presence of mucosal lesions cannot be reliably excluded based on this modality alone, and further small-bowel endoscopy should be considered in symptomatic patients. Video capsule endoscopy or device-assisted enteroscopy can be used, with device-assisted enteroscopy being preferred in stricturing Crohn's disease because of the risk of capsule retention or in patients in whom small-bowel malignancy is a possibility.
Conclusions: Endoscopy remains the criterion standard for the assessment of mucosal healing. Several alternative diagnostic modalities have become available that can be of value in specific clinical circumstances, particularly in patients with small-bowel involvement.
Copyright © 2015 American Society for Gastrointestinal Endoscopy. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Potential Conflicts and Disclosures: PSD has received research support from Alpco and Polymedco. BGL has served as a consultant for Takeda, Abbvie, and Nestle health sciences. BGF has received research support from, participated on scientific advisory boards, and served as a consultant for Abbott/Abbvie, Amgen, Astra Zeneca, Bristol-Myers Squibb, Janssen, Pfizer, Tillotts, and UCB Pharma; has participated on scientific advisory boards and served as a consultant for Avaxia Biologics Inc., Celgene, Biogen, Ferring, Merck, Novonordisk, Prometheus, Protagonist, Salix, Takeda, TiGenix, and Teva; has received research support and served as a consultant for Roche/Genentech, Millennium, and Receptos; has received research support from Santarus and Sanofi; has served on scientific advisory boards for Novartis, has served as a consultant forActogenix, Albireo Pharma, Avir Pharma, Axcan, Baxter Healthcare Corp., Boehringer-Ingelheim, Calypso Biotech, EnGene, , GiCare Pharma, Gilead, Given Imaging Inc., GSK, Ironwood Pharma, Kyowa Kakko Kirin Co Ltd., Lexicon, Lilly, Nektar, Serono, Shire, Sigmoid Pharma, Synergy Pharma Inc., Vertex Pharma, VHsquared Ltd., Warner-Chilcott, Wyeth, Zealand, Zyngenia; has participated in speakers bureaus for Abbott/AbbVie, JnJ/Janssen, Takeda, Warner-Chilcott, UCB Pharma; and is on the board of directors for Robarts Clinical Trials. GDH has received research support and lecture fees from, and served as a consultant for Abbvie, Janssen and Takeda; has served as a consultant for and received lecture fees from Centocor, Ferring, Giuliani SpA, Merck, Otsuka, Shire, Schering-Plough, Tillotts, UCB, and Vifor; has received research support from Given Imaging, MSD, DrFalk Pharma, and Photopill; has served as a consultant for Ablynx, ActoGeniX, AM Pharma, Boehringer Ingelheim GmbH, ChemoCentryx, Cosmo Technologies, Elan Pharmaceuticals, Engene, Dr Falk Pharma, Galapagos, Given Imaging, GlaxoSmithKline, Mitsubishi Tanabe Pharma, Neovacs, Novonordisk, PDL Biopharma, Pfizer, Receptos, Salix, Sandoz, Setpoint, Sigma, Versant; and has received lecture fees from Norgine, and Tramedico. WJS has received research support from Janssen, Abbvie, and Western University London Ontario (owner of Robarts Clinical Trials); and has served as a consultant for Janssen, Abbvie, UCB Pharma, Shire, Salix, and Takeda
Figures
References
-
- Ordas I, Eckmann L, Talamini M, et al. Ulcerative colitis. Lancet 2012;380:1606–19. - PubMed
-
- Baumgart DC, Sandborn WJ. Crohn’s disease. Lancet 2012;380:1590–605. - PubMed
-
- Williet N, Sandborn WJ, Peyrin-Biroulet L. Patient-reported outcomes as primary end points in clinical trials of inflammatory bowel disease. Clin Gastroenterol Hepatol 2014;12:1246–56.e6. - PubMed
-
- Peyrin-Biroulet L, Reinisch W, Colombel JF, et al. Clinical disease activity, C-reactive protein normalisation and mucosal healing in Crohn’s disease in the SONIC trial. Gut 2014;63:88–95. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
