

Transvaginal morcellation
- PMID: 26005318
- PMCID: PMC4432719
- DOI: 10.4293/JSLS.2014.00255
Transvaginal morcellation
Abstract
Background and objectives: Transvaginal uterine morcellation has been described in the literature for more than a century. Despite an extensive body of literature documenting its safety and feasibility, concerns about morcellating occult malignant entities have raised questions regarding this technique. In this study, we looked at a single teaching institution's experience with transvaginal morcellation for leiomyomatous uteri. In addition, we reviewed the published literature for outcomes associated with transvaginal morcellation techniques.
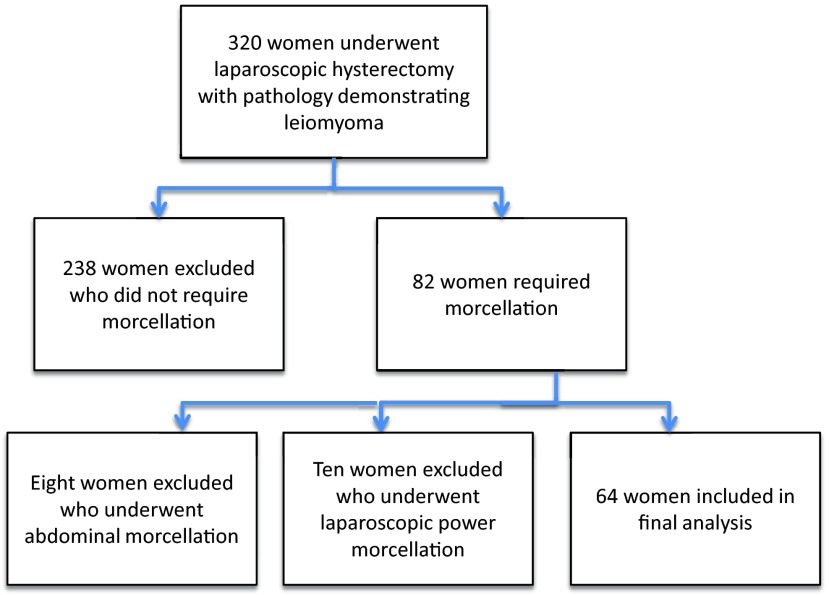
Methods: This study was a retrospective case series. Charts of women who underwent total laparoscopic hysterectomy, robot-assisted laparoscopic hysterectomy, and laparoscopic-assisted vaginal hysterectomy for leiomyoma from July 1, 2011, through December 31, 2013, were reviewed. Cases were included if transvaginal morcellation was performed. Morcellation was performed by bringing the uterus into the vagina and by performing a wedge resection technique to reduce the volume of the specimen. Baseline demographics and intra- and postoperative outcomes were abstracted from the charts. A PubMed search from January 1, 1970 to October 31, 2014 was performed to review the literature regarding transvaginal morcellation.
Results: Sixty-four women who underwent laparoscopy for leiomyomatous uteri with transvaginal morcellation were identified from July 1, 2011 through December 31, 2013. Mean operative time was 210 minutes (SD 75.5; range, 93-420). The mean blood loss was 153 mL (SD 165; range, 25-1000). The mean uterine size was 608 g (SD 367; range, 106-1834). There were no surgical complications directly attributed to morcellation. The literature search yielded 22 articles describing outcomes after transvaginal morcellation, with a total of 1953 morcellated specimens.
Conclusions: Transvaginal uterine morcellation appears to be a safe alternative to laparotomy for the removal of large uterine specimens in select patients.
Keywords: Fibroid; Laparoscopic abdominal vaginal hysterectomy; Leiomyoma; Transvaginal morcellation.
References
-
- Wu JM, Wechter ME, Geller EJ, Nguyen TV, Visco AG. Hysterectomy rates in the United States, 2003. Obstet Gynecol. 2007;110:1091–1095. - PubMed
-
- Kluivers KB, Johnson NP, Chien P, Vierhout ME, Bongers M, Mol BW. Comparison of laparoscopic and abdominal hysterectomy in terms of quality of life: a systematic review. Eur J Obstet Gynecol Reprod Biol. 2008;136:3–8. - PubMed
-
- Pelosi MA, Pelosi MA. The Pryor technique of uterine morcellation. Int J Gyenaecol Obstet. 1997;58:299–303. - PubMed
-
- Steiner RA, Wight E, Tadir Y, Haller U. Electrical cutting device for laparoscopic removal of tissue from the abdominal cavity. Obstet Gynecol. 1993;81:471–474. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical