

Economic burden of opioid-induced constipation among long-term opioid users with noncancer pain
- PMID: 26005516
- PMCID: PMC4437482
Economic burden of opioid-induced constipation among long-term opioid users with noncancer pain
Abstract
Background: Opioid-induced constipation (OIC) can be a debilitating side effect of opioid therapy and may result in increased medical costs. The published data on the economic burden of OIC among long-term opioid users are limited.
Objective: To assess the economic burden of OIC in patients with noncancer pain in a managed care population in the United States.
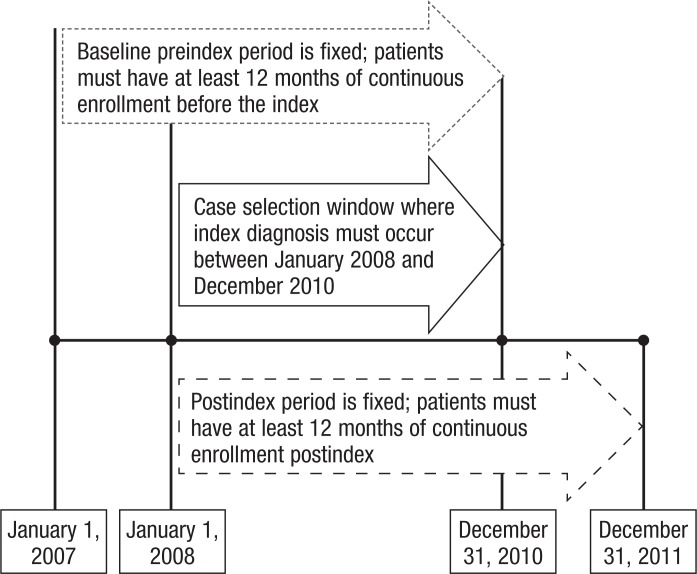
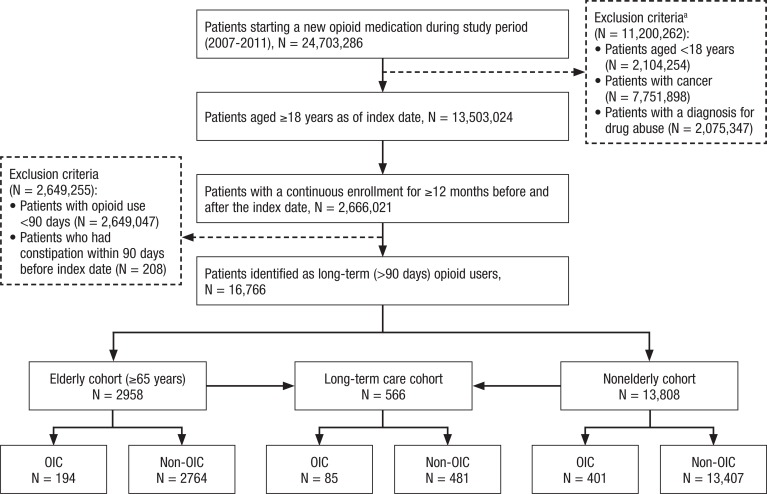
Methods: This retrospective study used 2007-2011 data from the Truven Health MarketScan Commercial and Medicare databases. The study included adults with ≥12 months of insurance enrollment before and after starting long-term (≥90 days) use of opioids. Patients were excluded if they had cancer or a diagnosis of drug abuse or drug dependence during the study period, or if they had constipation or bowel obstruction within 90 days before starting opioid therapy during the study period. OIC was identified by International Classification of Diseases, Ninth Edition codes for constipation (564.0) or bowel obstruction (560.x) within 12 months of the initiation of an opioid. Patients with OIC were identified in the nonelderly, elderly (age ≥65 years), and long-term care populations. Differences in costs and healthcare resource utilization were calculated using propensity scoring.
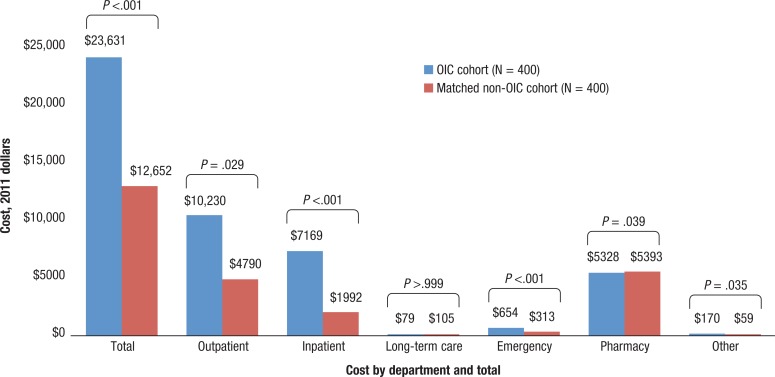
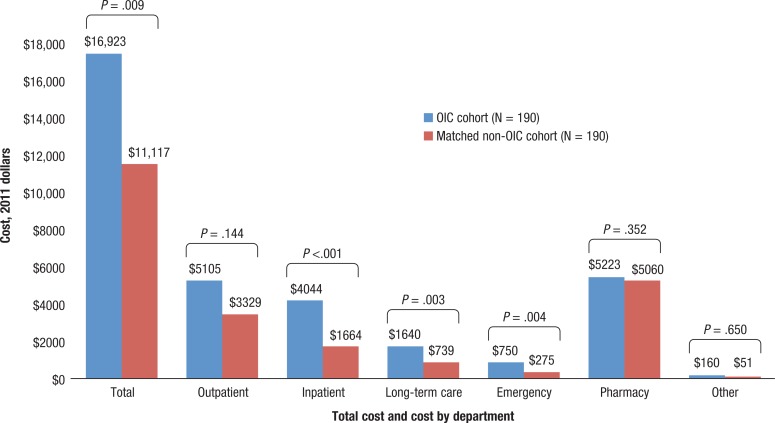
Results: A total of 13,808 nonelderly (age, 48.6 ± 10.4 years; female, 50%) and 2958 elderly patients (age, 78.7 ± 8.1 years; female, 70%) met the study inclusion criteria. Of 401 nonelderly and 194 elderly patients with OIC, 85 patients initiated opioid therapy in a long-term care facility (age, 80.7 ± 11.6 years; female, 77%). After matching by key covariates, patients with OIC had significantly more hospital admissions than patients without OIC (nonelderly, 33% vs 22%, respectively; P <.001; elderly, 51% vs 31%, respectively; P <.001) and longer inpatient stays (nonelderly, 3.0 ± 8.4 days vs 1.0 ± 3.0 days, respectively; P <.001; elderly, 5.2 ± 12.2 days vs 2.1 ± 4.0 days, respectively; P <.001). The group with OIC had significantly higher total healthcare costs than the group without OIC in all 3 study cohorts (nonelderly, $23,631 ± $67,209 vs $12,652 ± $19,717, respectively; elderly, $16,923 ± $38,191 vs $11,117 ± $19,525, respectively; long-term care, $16,000 ± $22,897 vs $14,437 ± $25,690, respectively; all P <.05).
Conclusion: To the best of our knowledge, this is the first study to analyze the economic impact of long-term use of opioids among patients with OIC, using real-world data. The findings underscore the significant economic burden associated with long-term opioid use for noncancer pain in a managed care population. Effective therapies for OIC may reduce the associated economic burden and improve quality of life for long-term opioid users.
Keywords: constipation; economic burden; elderly; healthcare resource utilization; long-term care; long-term opioid use; opioid-induced constipation; pain management.
Figures
References
-
- Trescot A, Glaser SE, Hansen H. Effectiveness of opioids in the treatment of chronic non-cancer pain. Pain Physician. 2008; 11: S181–S200. - PubMed
-
- Dorn SD, Meek PD, Shah ND. Increasing frequency of opioid prescriptions for chronic abdominal pain in US outpatient clinics. Clin Gastroenterol Hepatol. 2011; 9: 1078–1085.e1. Erratum in: Clin Gastroenterol Hepatol. 2012; 10: 332. - PubMed
-
- Bell T, Milanova T, Grove G, et al. OBD symptoms impair quality of life and daily activities, regardless of frequency and duration of opioid treatment: results of a US patient survey (PROBE survey). J Pain. 2007; 8(4 suppl 1). Abstract 882.
-
- Singh G, Kahler K, Bharathi V, et al. Constipation in adults: complications and comorbidities. Gastroenterology. 2005; 128(4 suppl 2). Abstract S960.
LinkOut - more resources
Full Text Sources
Miscellaneous