Ultra high resolution optical coherence tomography in Boston type I keratoprosthesis
- PMID: 26005549
- PMCID: PMC4424714
- DOI: 10.4103/2008-322X.156092
Ultra high resolution optical coherence tomography in Boston type I keratoprosthesis
Abstract
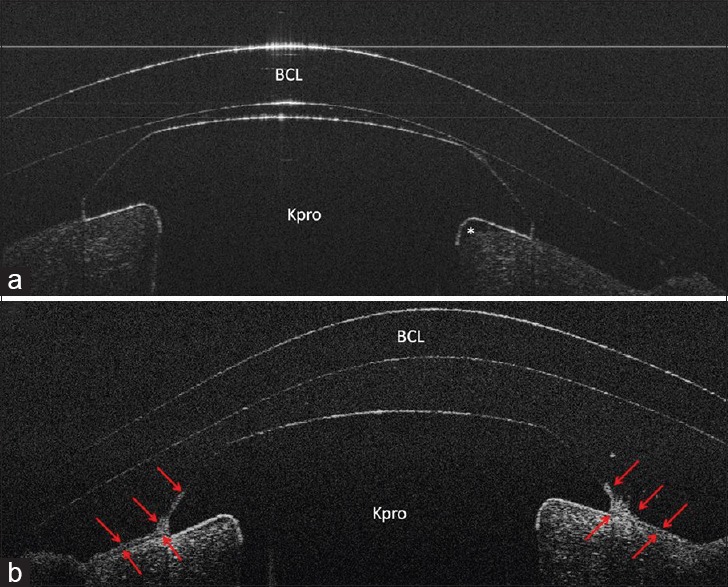
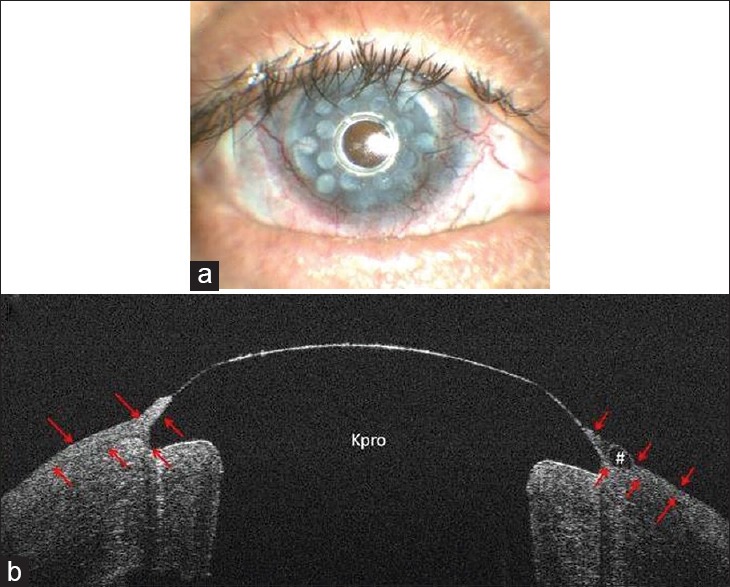
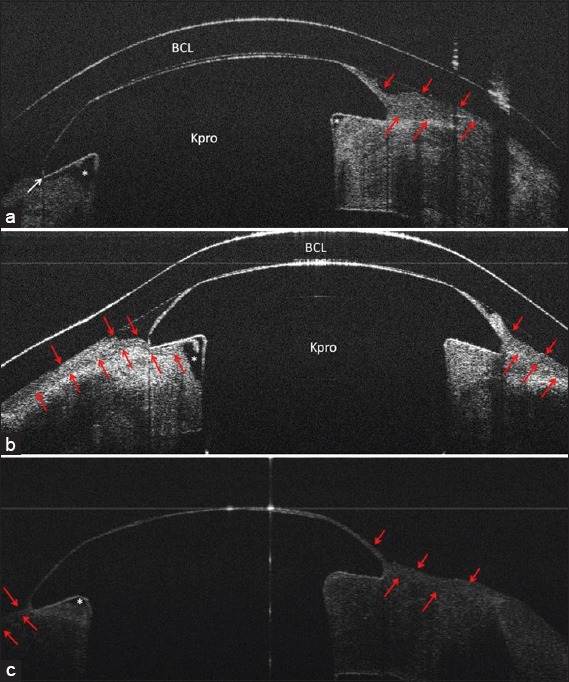
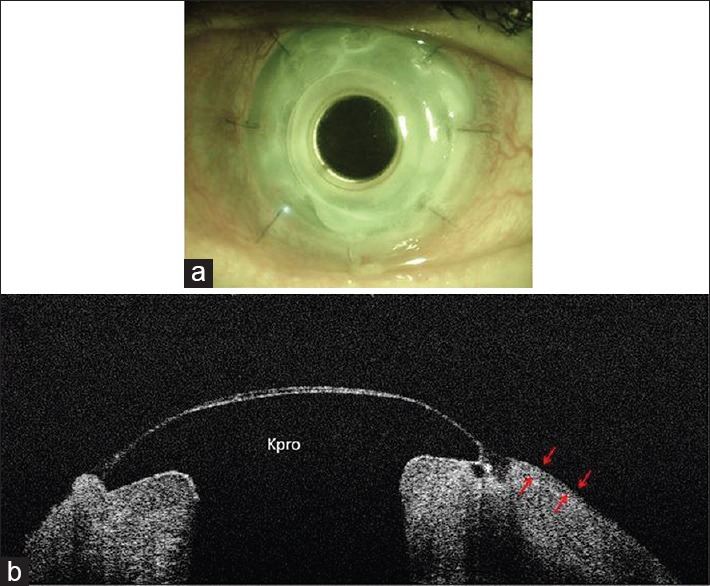
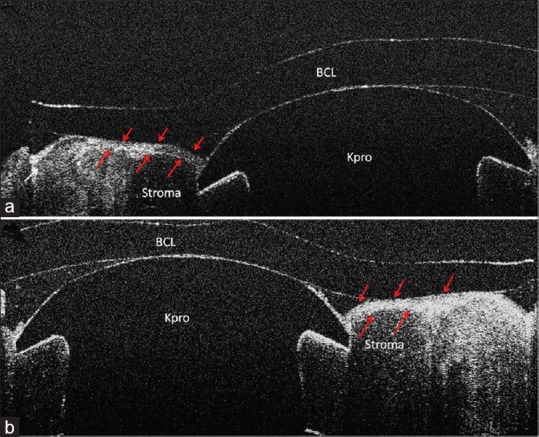
Purpose: To evaluate the anterior keratoprosthesis-cornea interface in eyes with Boston type I keratoprosthesis (Kpro).
Methods: In a prospective non-interventional study, patients with Boston type I Kpro underwent ultra-high resolution optical coherence tomography (UHR-OCT) evaluation. The images were used to measure and describe characteristics of the anterior keratoprosthesis-cornea interface, epithelial interaction at the keratoprosthesis edge and the keratoprosthesis-cornea interface gap.
Results: Ten patients including 4 male and 6 female subjects with different preoperative diagnoses, i.e. 8 multiple corneal graft failures and 2 immunological ocular surface diseases, were studied. Mean age was 62.1 ± 20.0 (range, 33.0-83.0) years and mean interval between surgery and UHR-OCT evaluation was 15.2 ± 11.09 months. In eight patients, 360° epithelial growth over the peripheral edge of the Kpro was documented. We detected keratoprosthesis-cornea interface gap in three patients. One subject had developed postoperative endophthalmitis 8 months after surgery and the other two cases were among the high risk group according to the preoperative diagnosis. In one patient with severe ocular hypotony, the Kpro edge was inserted into the anterior stroma and covered with epithelium.
Conclusion: UHR-OCT showed that corneal epithelium covers the Kpro edge and seals the potential space between the Kpro and cornea in 80% of cases. The presence of a gap in the interface and lack of epithelial sealing around the Kpro edge might be associated with endophthalmitis.
Keywords: Anterior Segment OCT; Boston Type I Keratoprosthesis; Ultra High-resolution OCT.
Conflict of interest statement
Figures
References
-
- Aldave AJ, Kamal KM, Vo RC, Yu F. The Boston type I keratoprosthesis: Improving outcomes and expanding indications. Ophthalmology. 2009;116:640–651. - PubMed
-
- Zerbe BL, Belin MW, Ciolino JB. Boston Type 1 Keratoprosthesis Study Group. Results from the multicenter Boston Type 1 Keratoprosthesis Study. Ophthalmology. 2006;113:1779.e1–7. - PubMed
-
- Bradley JC, Hernandez EG, Schwab IR, Mannis MJ. Boston type 1 keratoprosthesis: The university of california davis experience. Cornea. 2009;28:321–327. - PubMed
-
- Shousha MA, Karp CL, Perez VL, Hoffmann R, Ventura R, Chang V, et al. Diagnosis and management of conjunctival and corneal intraepithelial neoplasia using ultra high-resolution optical coherence tomography. Ophthalmology. 2011;118:1531–1537. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous