

Lateral orbitotomy approach for removing hyperostosing en plaque sphenoid wing meningiomas. Description of surgical strategy and analysis of findings in a series of 88 patients with long-term follow up
- PMID: 26005574
- PMCID: PMC4434495
- DOI: 10.4103/2152-7806.157074
Lateral orbitotomy approach for removing hyperostosing en plaque sphenoid wing meningiomas. Description of surgical strategy and analysis of findings in a series of 88 patients with long-term follow up
Abstract
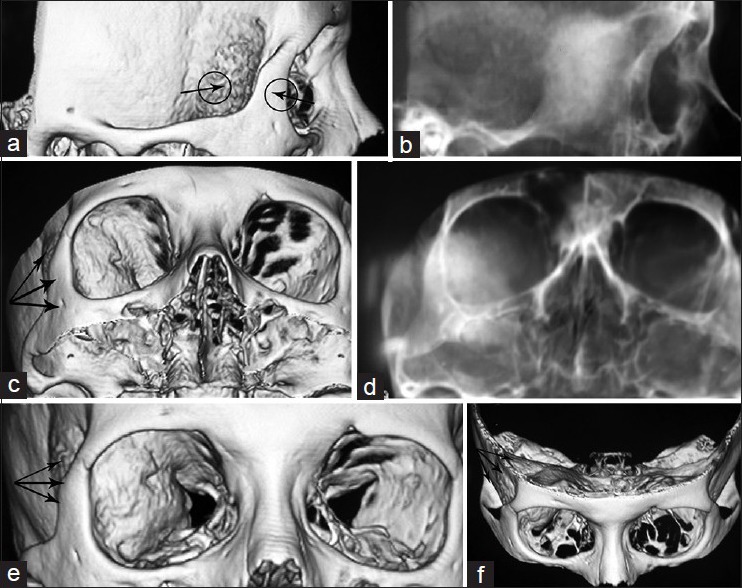
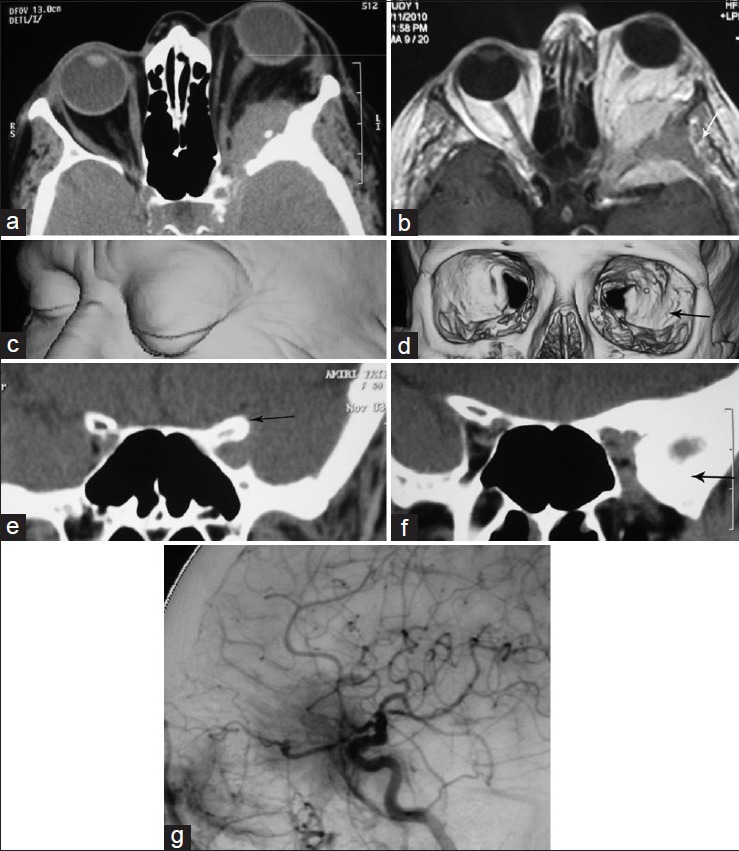
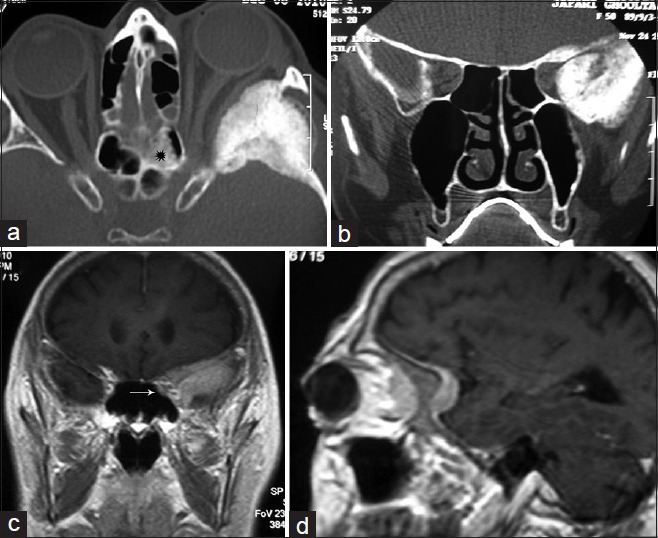
Background: Sphenoid wing meningiomas extending to the orbit (ePMSW) are currently removed through several transcranial approaches. Presenting the largest surgical cohort of hyperostosing ePMSW with the longest follow up period, we will provide data supporting minilateral orbitotomy with excellent exposure for wide resection of all compartments of the tumor.
Methods: A retrospective survival analysis is made of the data cumulated prospectively during a period of 34 years, including 88 cases of ePMSW with a mean follow up period of 136.4 months. The impact of preoperative variables upon different outcome measures is evaluated. Standard pterional craniotomy was performed in 12 patients (C) while the other 76 cases underwent the proposed modified lateral miniorbitotomy (LO).
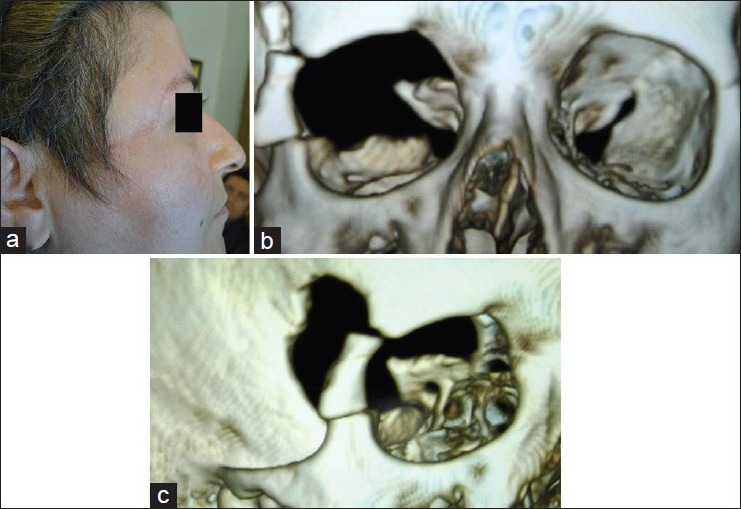
Results: There were 31 men and 57 women. The age range varied between 12 and 70 years. Patients presented with unilateral exophthalmos (Uex) ranging between 3 and 16 mm. Duration of proptosis before operation varied between 6 months and 16 years. The status of visual acuity (VA) prior to operation was: no light perception (NLP) in 16, light perception (LP) up to 0.2 in 3, 0.3-0.5 in 22, 0.6-0.9 in 24, and full vision in 23 patients. Postoperatively, acceptable cosmetic appearance of the eyes was seen in 38 cases and in 46 mild inequality of < 2 mm was detected. Four cases had mild enophthalmos (En). Among those who had the worst VA, two improved and one became almost blind after operation. The cases with VA in the range of 0.3-0.5 improved. Among those with good VA (0.5 to full vision), 2 became blind, vision diminished in 10, and improved or remained full in the other 35 cases. Tumor recurrence occurred in 33.3% of group C and 10.5% of group LO (P = 0.05). The major determinant of tumor regrowth was the technique of LO (P = 0.008).
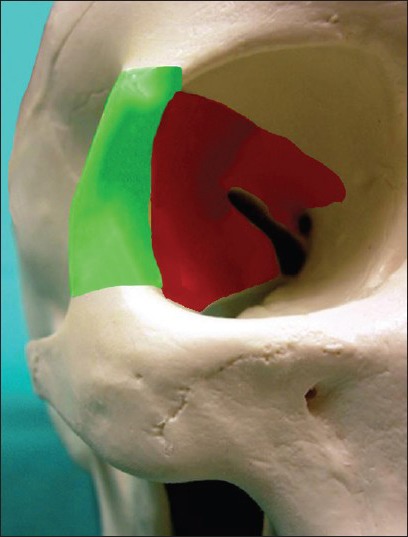
Conclusion: Using LO technique, the risky corners involved by the tumor is visualized from the latero-inferior side rather than from the latero-superior avenue. This is the crucial milestone to achieve aggressive removal of all the involved compartments of the lesion. Satisfactory cosmetic result is reported using mini LO technique after widely exposing and removing the hyperostotic bone down to the subtemporal fossa with only simple repair of the dura without cranioplasty.
Keywords: Lateral orbitotomy; meningioma; orbital tumors; proptosis; spheno-orbital meningioma; sphenoid wing meningioma; unilateral exophthalmos..
Figures


References
-
- Abbott KH, Glass B. Pterional meningioma en plaque: Report of a case of thirty-six years’ duration. J Neurosurg. 1955;12:50–2. - PubMed
-
- Al-Mefty O. Supraorbital-pterional approach to skull base lesions. Neurosurgery. 1987;21:474–7. - PubMed
-
- Arai H, Sato K, Katsuta T, Rhoton AL. Lateral approach to intraorbital lesions: Anatomic and surgical considerations. Neurosurgery. 1996;39:1157–63. - PubMed
-
- Baldeschi L, MacAndie K, Hintschich C, Wakelkamp IM, Prummel MF, Wiersinga WM. The removal of the deep lateral wall in orbital decompression: Its contribution to exophthalmos reduction and influence on consecutive diplopia. Am J Ophthalmol. 2005;140:642–7. - PubMed
-
- Bikmaz K, Mrak R, Al-Mefty O. Management of bone-invasive, hyperostotic sphenoid wing meningiomas. J Neurosurg. 2007;107:905–12. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials