

Radiosurgery for symptomatic cavernous malformations: A multi-institutional retrospective study in Japan
- PMID: 26005588
- PMCID: PMC4434491
- DOI: 10.4103/2152-7806.157071
Radiosurgery for symptomatic cavernous malformations: A multi-institutional retrospective study in Japan
Abstract
Background: A group study for symptomatic cavernous malformation (CM) treated with gamma knife (GK) surgery was performed.
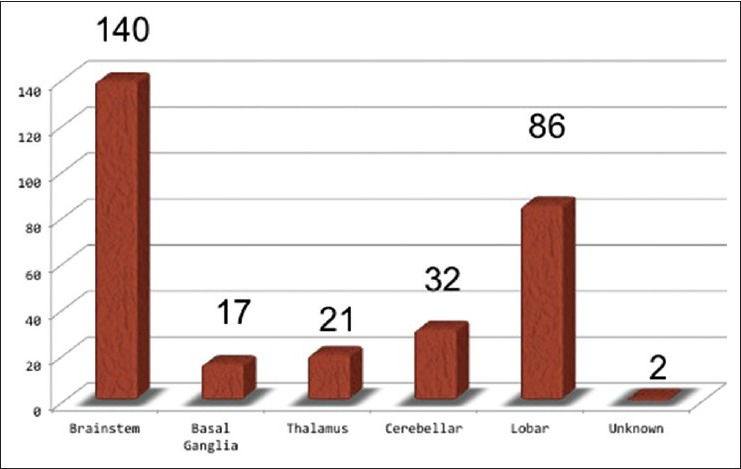
Methods: A total of 298 cases collected from 23 GK centers across Japan were included. Hemorrhage was the most common manifestation, followed by seizures and neurological deficits. Most of the lesions were located in the brainstem and basal ganglia, followed by the cerebral or cerebellar hemispheres. The CMs, which had a mean diameter of 14.8 mm, were treated using GK surgery with a mean marginal dose of 14.6 Gy.
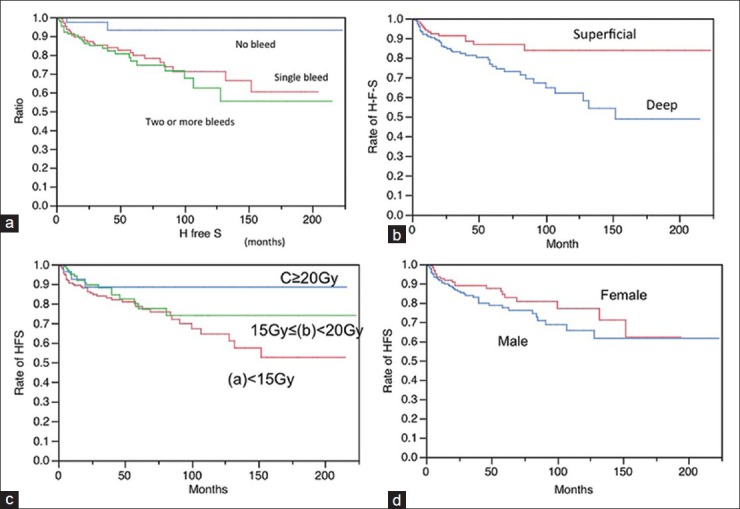
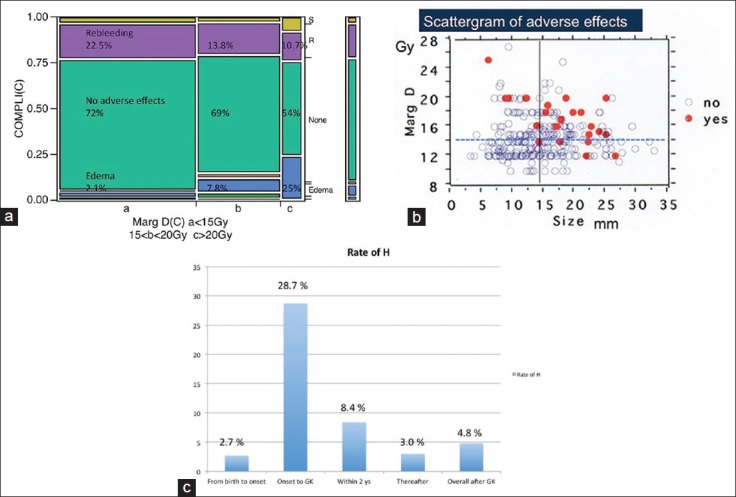
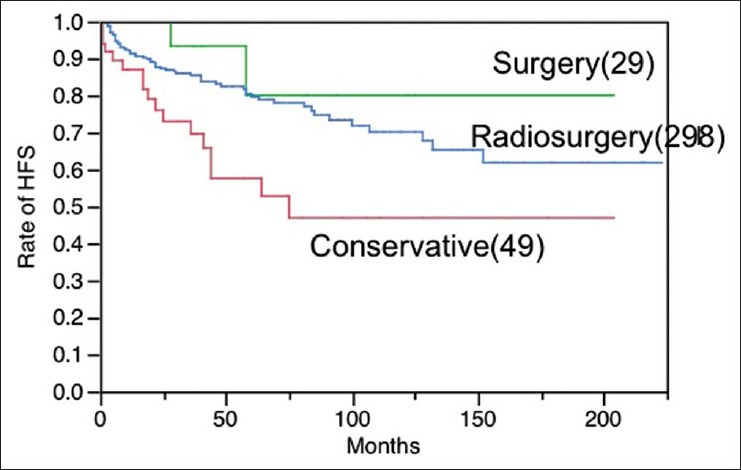
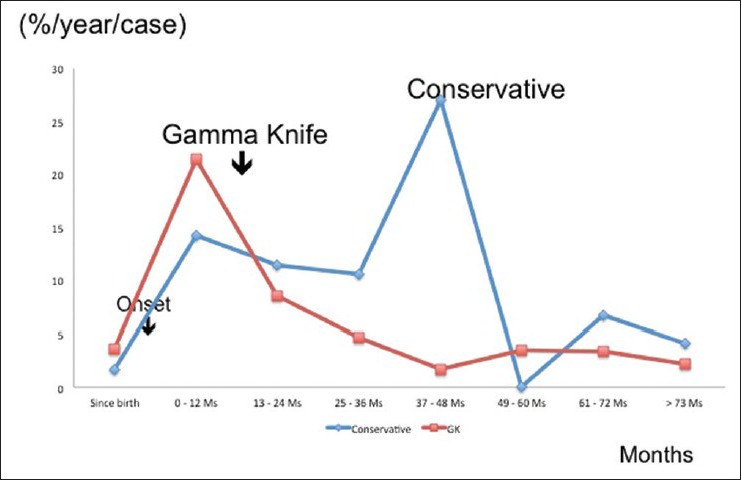
Results: In terms of hemorrhage-free survival (HFS), a marked dissociation was confirmed between the hemorrhage and seizure groups, while no obvious difference was noted between sexes. Superficial CMs located in cerebellum or lobar regions responded to the treatment better than deeply located CMs in the basal ganglia or brainstem. No significant difference of dose-dependent response was seen for three different ranges of marginal dose: Less than 15 Gy, between 15 and 20 Gy, and more than 20 Gy. Complications were more frequent after a marginal dose of over 15 Gy and in patients with lesions more than 15 mm in diameter. The rates of annual hemorrhage were estimated to be 7.4% during the first 2 years after radiosurgery and 2.8% thereafter. The overall hemorrhage rate after radiosurgery was 4.4%/year/patient.
Conclusion: The risk of hemorrhage is considerably reduced after GK treatment. The HFS as well as annual hemorrhage rate after GK treatment was apparently superior to that after conservative treatment for symptomatic CMs. To optimize the success of GK treatment, it is important to reduce the incidence of complications.
Keywords: Cavernous malformation; gamma knife; radiosurgery; symptomatic lesion; vascular anomaly.
Figures
Similar articles
-
Radiosurgery of intracranial cavernous malformations.Acta Neurochir (Wien). 2002 Sep;144(9):869-78; discussion 878. doi: 10.1007/s00701-002-0983-9. Acta Neurochir (Wien). 2002. PMID: 12376768
-
Significant Hemorrhage Rate Reduction after Gamma Knife Radiosurgery in Symptomatic Cavernous Malformations: Long-Term Outcome in 95 Case Series and Literature Review.Stereotact Funct Neurosurg. 2017;95(6):369-378. doi: 10.1159/000480664. Epub 2017 Nov 4. Stereotact Funct Neurosurg. 2017. PMID: 29131117 Review.
-
Contemporary radiosurgery of cerebral cavernous malformations: Part 2. Treatment outcome for hemispheric lesions.J Neurosurg. 2018 Jul 27;130(6):1826-1834. doi: 10.3171/2018.2.JNS171267. Print 2019 Jun 1. J Neurosurg. 2018. PMID: 30052157
-
Gamma knife radiosurgery for cavernous malformations: a comprehensive study on symptom relief, hemorrhage rates, and histopathological changes.Neurosurg Rev. 2025 Jan 30;48(1):106. doi: 10.1007/s10143-025-03257-y. Neurosurg Rev. 2025. PMID: 39883199 Free PMC article.
-
Stereotactic radiosurgery for the treatment of symptomatic brainstem cavernous malformations.Neurosurg Focus. 2010 Sep;29(3):E11. doi: 10.3171/2010.7.FOCUS10151. Neurosurg Focus. 2010. PMID: 20809752 Review.
Cited by
-
Prognostic Factors Analysis for Intracranial Cavernous Malformations Treated with Linear Accelerator Stereotactic Radiosurgery.Life (Basel). 2022 Aug 31;12(9):1363. doi: 10.3390/life12091363. Life (Basel). 2022. PMID: 36143399 Free PMC article.
-
Treatment of Cerebral Cavernous Malformations Presenting With Seizures: A Systematic Review and Meta-Analysis.Front Neurol. 2020 Oct 26;11:590589. doi: 10.3389/fneur.2020.590589. eCollection 2020. Front Neurol. 2020. PMID: 33193057 Free PMC article.
-
Long-Term Outcomes of Gamma Knife Radiosurgery for Cerebral Cavernous Malformations: 10 Years and Beyond.J Korean Med Sci. 2024 Aug 19;39(32):e229. doi: 10.3346/jkms.2024.39.e229. J Korean Med Sci. 2024. PMID: 39164054 Free PMC article.
-
Childhood stroke.Nat Rev Dis Primers. 2022 Feb 24;8(1):12. doi: 10.1038/s41572-022-00337-x. Nat Rev Dis Primers. 2022. PMID: 35210461 Review.
-
Radiosurgery effects and adverse effects in symptomatic eloquent brain-located Cavernomas.J Radiat Res. 2023 Jan 20;64(1):133-141. doi: 10.1093/jrr/rrac056. J Radiat Res. 2023. PMID: 36208871 Free PMC article.
References
-
- Amin-Hanjani S, Ogilvy CS, Candia GJ, Lyons S, Chapman PH. Stereotactic radiosurgery for cavernous malformations: Kjellberg's experience with proton beam therapy in 98 cases at the Harvard cyclotron. Neurosurgery. 1998;42:1229–38. - PubMed
-
- Barker FG, II, Amin-Hanjani S, Butler WE, Lyons S, Ojemann RG, Chapman PH, et al. Temporal clustering of hemorrhages from untreated cavernous malformation of the central nervous system. Neurosurgery. 2001;49:15–25. - PubMed
-
- Bertalanffy H, Gilsbach JM, Eggert HR, Seeger W. Microsurgery of deep-seated cavernous angiomas: Report of 26 cases. Acta Neurochir (Wien) 1991;108:91–9. - PubMed
-
- Chang SD, Levy RP, Adler JR, Martin DP, Krakovitz PR, Steinberg GK. Stereotactic radiosurgery of angiographically occult vascular malformations: 14-year experience. Neurosurgery. 1998;43:213–21. - PubMed
-
- Cohen DS, Zubay GP, Goodman RR. Seizure outcome after lesionectomy for cavernous malformations. J Neurosurg. 1995;83:237–42. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources