

Migration of endotacker into the bladder 7 years after laparoscopic retroperitoneal Burch application
- PMID: 26005983
- PMCID: PMC4752106
- DOI: 10.1590/S1677-5538.IBJU.2015.02.28
Migration of endotacker into the bladder 7 years after laparoscopic retroperitoneal Burch application
Abstract
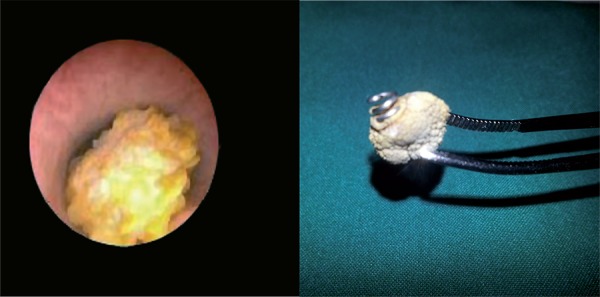
Laparoscopy began to be used widely since the second half of 1990s as an alternative to laparotomy or vaginal approaches in incontinence and pelvic diseases in women, based on its claimed better success rates. Injuries were reported in the bladder, gastrointestinal system and the entry of the Verress cannula in early and late laparoscopic applications. De-novo urging, voiding dysfunctions, marked recurrences and surgical inefficiencies were observed in 5-year follow-ups after laparoscopic incontinence surgery. Although tension-free midurethral sling operations replaced open laparoscopic colposuspensions nowadays, laparoscopic colposuspension is still preferred in cases where simultaneous laparoscopic paravaginal repair or sacrocolpopexy is considered or where synthetic graft implantation is contraindicated. Moreover, meshes and endotackers are still frequently used in many laparoscopic applications in various clinics. The migration of the tacker used in mesh fixation in a patient where retroperitoneal laparoscopic Burch was performed 7 years ago due to stress urinary incontinence and the extraction of the ossified tacker from the bladder will be presented.
Conflict of interest statement
Figures




Comment in
-
Re: Migration of endotacker into the bladder 7 years after laparoscopic retroperitoneal Burch application.Int Braz J Urol. 2015 Jul-Aug;41(4):821. doi: 10.1590/S1677-5538.IBJU.2015.0273. Int Braz J Urol. 2015. PMID: 26401880 Free PMC article. No abstract available.
Similar articles
-
Re: Migration of endotacker into the bladder 7 years after laparoscopic retroperitoneal Burch application.Int Braz J Urol. 2015 Jul-Aug;41(4):821. doi: 10.1590/S1677-5538.IBJU.2015.0273. Int Braz J Urol. 2015. PMID: 26401880 Free PMC article. No abstract available.
-
A surgical technique to adjust bladder neck suspension in laparoscopic Burch colposuspension.J Minim Invasive Gynecol. 2006 Jul-Aug;13(4):289-95. doi: 10.1016/j.jmig.2006.03.019. J Minim Invasive Gynecol. 2006. PMID: 16825068
-
Laparoscopic TOT-like Burch Colposuspension: Back to the Future?J Minim Invasive Gynecol. 2021 Jan;28(1):24-25. doi: 10.1016/j.jmig.2020.04.018. Epub 2020 Apr 24. J Minim Invasive Gynecol. 2021. PMID: 32339752
-
Burch Colposuspension.Urol Clin North Am. 2019 Feb;46(1):53-59. doi: 10.1016/j.ucl.2018.08.002. Urol Clin North Am. 2019. PMID: 30466702 Review.
-
Laparoscopic Burch colposuspension.Curr Opin Obstet Gynecol. 2007 Aug;19(4):314-8. doi: 10.1097/GCO.0b013e328216f75e. Curr Opin Obstet Gynecol. 2007. PMID: 17625411 Review.
Cited by
-
Re: Migration of endotacker into the bladder 7 years after laparoscopic retroperitoneal Burch application.Int Braz J Urol. 2015 Jul-Aug;41(4):821. doi: 10.1590/S1677-5538.IBJU.2015.0273. Int Braz J Urol. 2015. PMID: 26401880 Free PMC article. No abstract available.
References
-
- Guner H, Yildiz A, Erdem A, Erdem M, Tiftik Z, Yildirim M. Surgical treatment of urinary stress incontinence by a suburethral sling procedure using a Mersilene mesh graft. Gynecol Obstet Invest. 1994;37:52–55. - PubMed
-
- Vancaillie TG, Schuessler W. Laparoscopic bladderneck suspension. J Laparoendosc Surg. 1991;1:169–173. - PubMed
-
- Frick AC, Paraiso MF. Laparoscopic management of incontinence and pelvic organ prolapse. Clin Obstet Gynecol. 2009;52:390–400. - PubMed
-
- Bulent Tiras M, Sendag F, Dilek U, Guner H. Laparoscopic burch colposuspension: comparison of effectiveness of extraperitoneal and transperitoneal techniques. Eur J Obstet Gynecol Reprod Biol. 2004;116:79–84. - PubMed
-
- Miannay E, Cosson M, Lanvin D, Querleu D, Crepin G. Comparison of open retropubic and laparoscopic colposuspension for treatment of stress urinary incontinence. Eur J Obstet Gynecol Reprod Biol. 1998;79:159–166. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources