

doi: 10.1007/s00261-015-0429-5.
The subperitoneal space and peritoneal cavity: basic concepts
Affiliations
- PMID: 26006061
- PMCID: PMC4584112
- DOI: 10.1007/s00261-015-0429-5
Item in Clipboard
The subperitoneal space and peritoneal cavity: basic concepts
Abdom Imaging.
2015 Oct.
Abstract
The subperitoneal space and peritoneal cavity are two mutually exclusive spaces that are separated by the peritoneum. Each is a single continuous space with interconnected regions. Disease can spread either within the subperitoneal space or within the peritoneal cavity to distant sites in the abdomen and pelvis via these interconnecting pathways. Disease can also cross the peritoneum to spread from the subperitoneal space to the peritoneal cavity or vice versa.
Keywords: Anatomy; Peritoneal cavity; Subperitoneal space.
Figures
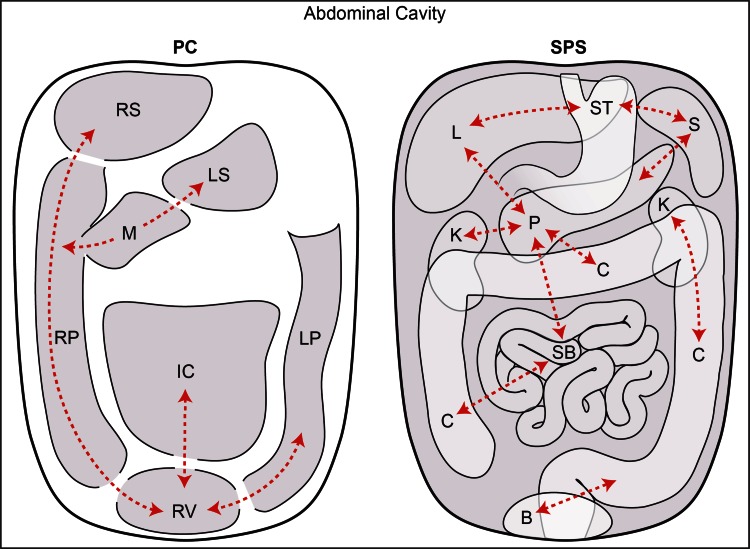
The peritoneal cavity vs the subperitoneal space. This is a schematic diagram showing the peritoneal cavity (PC) on the left and the subperitoneal space (SPS) on the right. The diagram illustrates that these are 2 completely separate spaces within the abdominal cavity. The peritoneal cavity and the subperitoneal space are separated by the peritoneum. The peritoneal cavity is one continuous space with interconnecting recesses, some of which are shown. The subperitoneal space is also one continuous space containing all the abdominal pelvic organs which are interconnected via ligaments and mesenteries. Dotted lines show some of these interconnections which allow for disease spread. Abbreviations for the peritoneal cavity: IC inframesocolic compartment, LP left paracolic recess, LS lesser sac, M Morison’s pouch, RP right paracolic recess, RS right subphrenic space, and RV rectovesical space. Abbreviations for the subperitoneal space: B bladder, C colon, K kidney, L liver, P pancreas, S spleen, SB small bowel, and ST stomach.
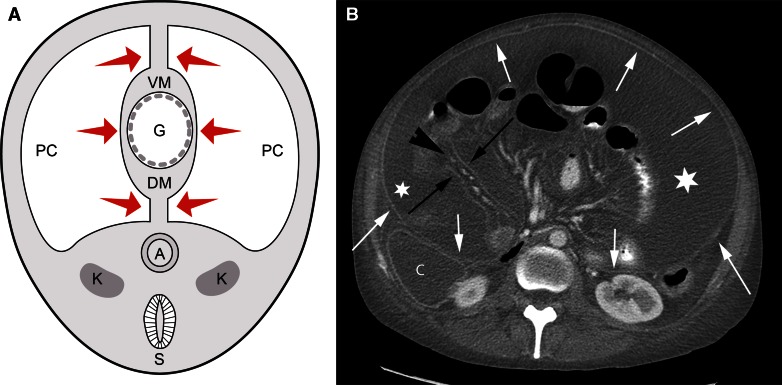
Relationship between the mesentery and the peritoneum. A Diagram of a 4-week-old embryo shows the coelomic cavity which will form the peritoneal cavity (PC) surrounding the primitive gut (G). The medial visceral layer (arrows) of the peritoneum is apposed on the gut and the mesentery, while the parietal layer is lateral. The dorsal mesentery (DM) conveys vessels from the aorta to the gut. Other than the peritoneal cavity, all the tissue in the abdominal cavity portion of the diagram is the subperitoneal space (light gray shaded area). Spine is shown on the diagram only for orientation purposes. A aorta, K kidney, S spine, and VM ventral mesentery. B Axial CT image shows the dorsal mesentery of the small bowel as subperitoneal tissue (arrowhead) between 2 layers of visceral peritoneum (black arrows). The parietal peritoneal reflection (white arrows) is also seen anterior to the colon (C), kidney, and in the anterior and lateral abdomen. There is fluid (asterisk) in the peritoneal cavity between the visceral (black arrows) and parietal (white arrows) layers of the peritoneum.
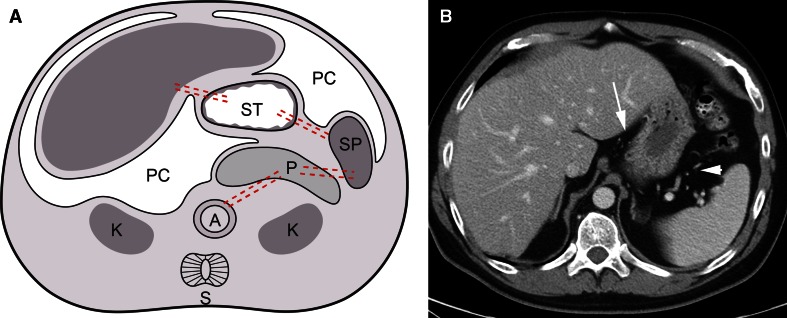
Abdominal ligaments. A Diagram showing development of an embryo. The liver develops in the ventral mesentery anterior to the stomach. The residual part of the ventral mesentery between the liver and stomach is called the gastrohepatic ligament in the adult. The spleen and pancreas form in the dorsal mesentery posterior to the stomach. The residual part of the dorsal mesentery between the spleen and stomach is called the gastrosplenic ligament in the adult. The pancreas fuses with the tissues anterior to the kidney to lie in the anterior pararenal space. The residual part of the dorsal mesentery between the spleen and pancreas is called the splenorenal ligament. Dotted lines approximate the paths of the ventral and dorsal mesenteries. A aorta, K kidney, L liver, PC peritoneal cavity, S spine, and ST stomach. Subperitoneal space = light gray shaded area in abdominal cavity portion of diagram. Spine is shown on the diagram only for orientation purposes. B Axial CT image of the upper abdomen shows the gastrohepatic (arrow) and gastrosplenic (arrowhead) ligaments containing the left gastric artery and short gastric vessels, respectively.
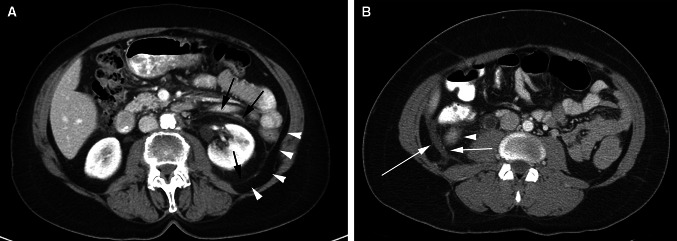
Renal fasciae. A Axial CT image shows the anterior and posterior renal fascia (black arrows). Arrowheads show the posterior pararenal space extending laterally as the properitoneal fat. B Axial CT image shows fluid (arrows) in between the 2 layers of the posterior renal fascia. Fluid from the anterior pararenal space can extend into this potential space between the 2 layers. Arrowhead points to the lower pole of the kidney.
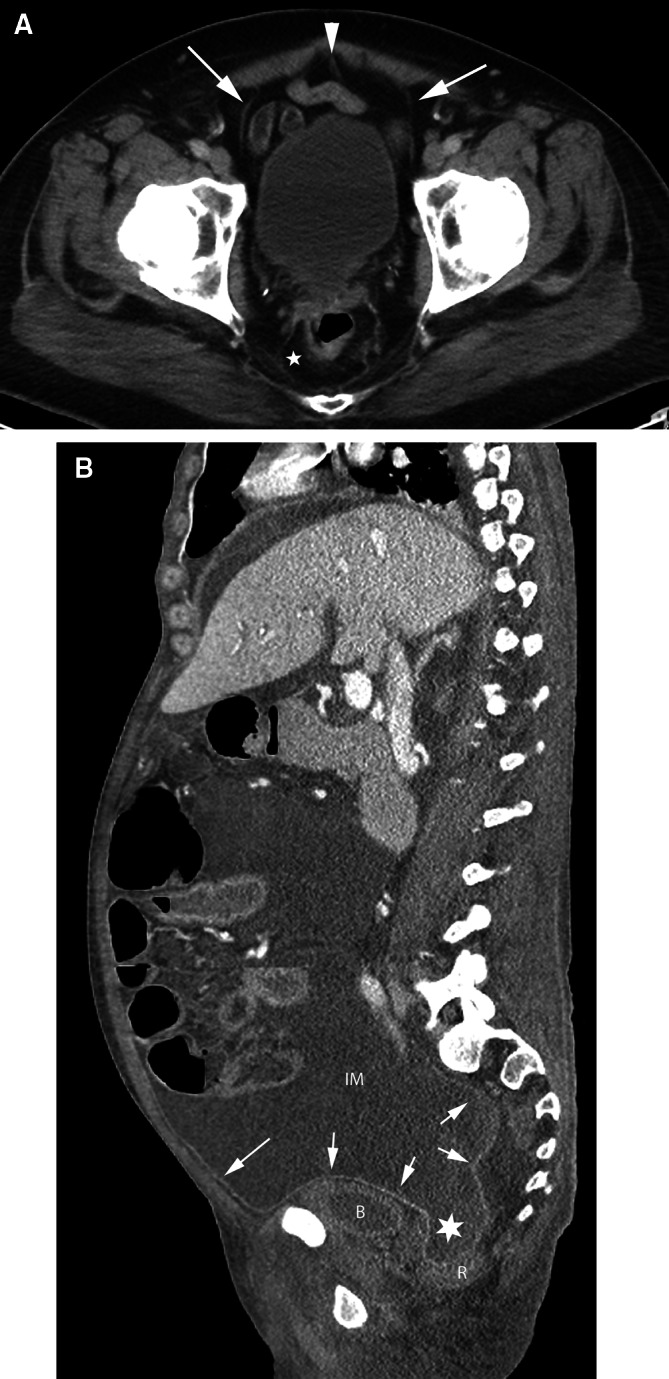
Pelvic spaces. A axial CT image of the pelvis. The urachus (arrowhead) and obliterated umbilical arteries (arrows) form the median umbilical ligament and the medial umbilical folds, respectively, and are encased within the umbilicovesical fascia forming the perivesical space. The prevesical space is anterior and lateral to the bladder. The perirectal space (asterisk) surrounds the rectum. B Sagittal CT image shows the peritoneum (arrows) along the anterior abdominal wall and reflecting over the bladder and rectum. Peritoneal fluid in the inframesocolic compartment (IM) communicates with the rectovesical recess (asterisk). The bladder is inferiorly displaced by the peritoneal fluid. B bladder, R rectum.
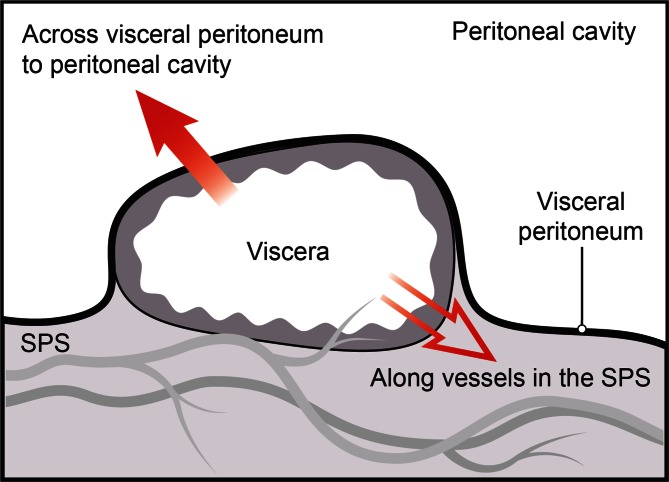
Diagram shows the 2 routes of disease spread for viscera which are covered by peritoneum–transperitoneal and subperitoneal. Disease can cross the visceral peritoneum (solid arrow) to enter and subsequently spread in the peritoneal cavity. Alternatively, disease can follow the vessels and lymphatics (open arrow) of the viscera to spread in the subperitoneal space (SPS).
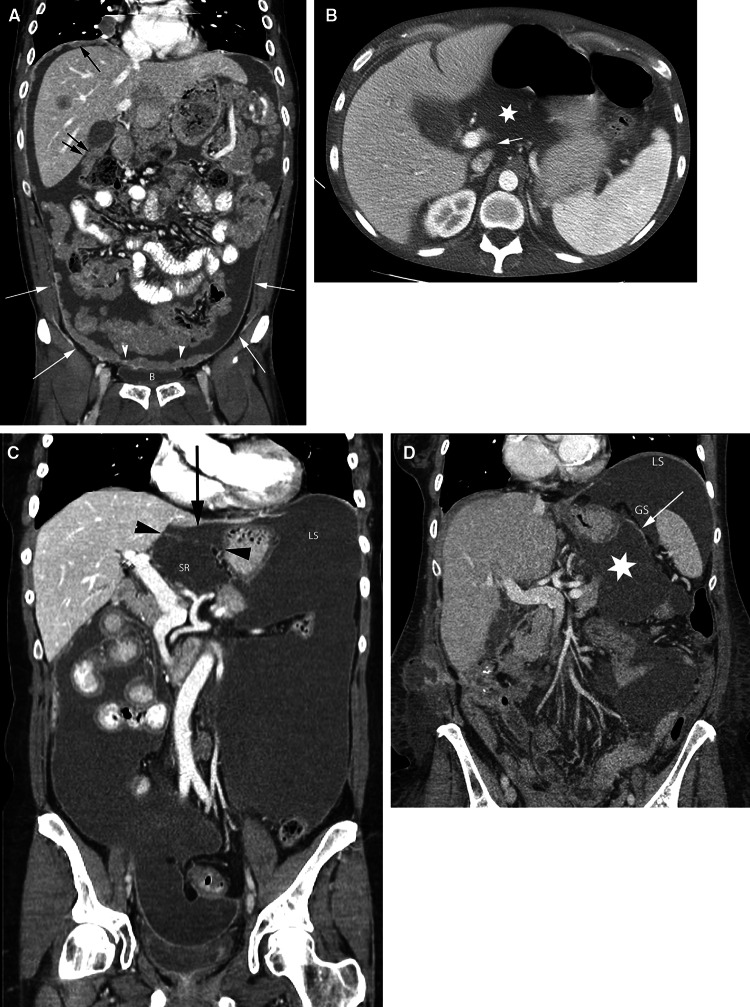
Peritoneal cavity fluid flow and recesses. A coronal CT image shows peritoneal carcinomatosis demonstrating the peritoneal recesses. Tumor in the right subdiaphragmatic recess (black arrow) and Morison’s pouch (double black arrows). Tumor (arrowheads) is also seen along the peritoneal reflection over the bladder (B). White arrows show continuity between the paravesical and paracolic recesses. B Axial CT image in a different patient shows the epiploic foramen (arrow) between the portal vein and inferior vena cava and fluid in the lesser sac (asterisk). C coronal CT image in a different patient shows fluid in the superior recess of the lesser sac (SR) and in the gastrohepatic recess (black arrow) separated by the gastrohepatic ligament (black arrowheads). Fluid in the gastrohepatic recess communicates with fluid in the left subphrenic space (LS). D coronal CT image in a different patient shows fluid in the lesser sac (asterisk) and in the gastrosplenic recess (GS) separated by the gastrosplenic ligament (arrow). There is continuity between the gastrosplenic and left subphrenic (LS) recesses.
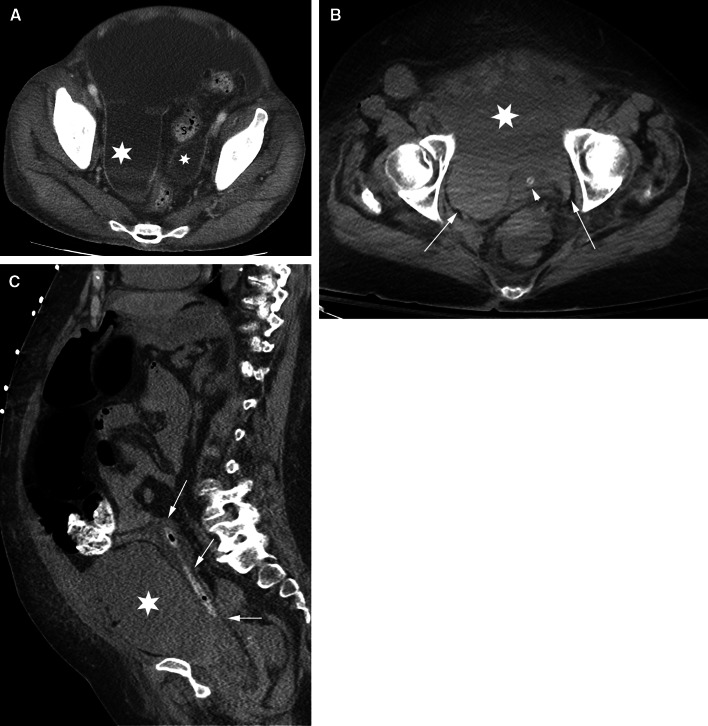
Pelvic intraperitoneal fluid vs extraperitoneal fluid. Pelvic fluid is shown in 2 different patients. The patient in A has intraperitoneal fluid. The patient in B and C has extraperitoneal fluid. A axial CT image shows intraperitoneal fluid in the right and left paravesical recesses (asterisks) lateral to the sigmoid colon (S) and superior to the bladder (not shown). B Axial CT image of a different patient shows extraperitoneal fluid in the prevesical space (asterisk) anterior to the decompressed bladder (arrowhead) containing a catheter. The bladder is displaced posteriorly. Fluid extends within the prevesical space (arrows) lateral to the bladder giving a “molar tooth” appearance. C sagittal CT image in the same patient as in B shows extraperitoneal fluid in the prevesical space (asterisk) anterior to the posteriorly displaced bladder (arrows) containing a catheter.

Extraperitoneal free air. Sagittal CT image shows pneumatosis of the ascending colon and extraluminal air in the adjacent mesentery (asterisk). This extraperitoneal free air tracks in the anterior and posterior pararenal spaces (arrows) to the bare area of the liver and diaphragm (arrowheads).
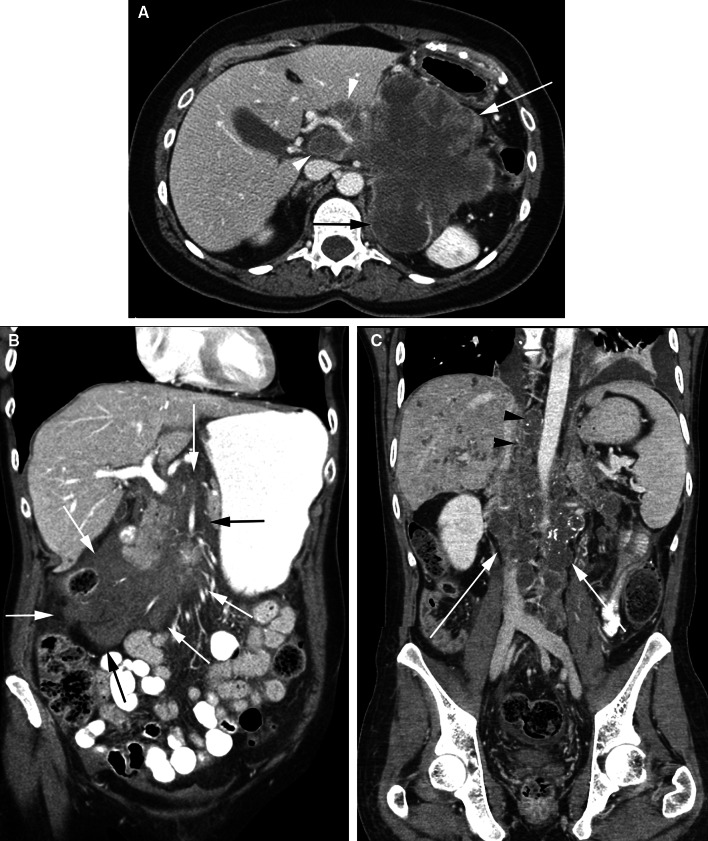
Subperitoneal spread of disease. A Axial CT image shows a large pancreatic mass (white arrow) extending along the hepatoduodenal ligament to the porta hepatis (arrowheads). Mass also invades the left perinephric space and engulfs the adrenal gland (black arrow). Superiorly, the mass extended into the gastrohepatic ligament with invasion of the left lobe of the liver (not shown). B Coronal CT image shows a hematoma in the root of the small bowel mesentery extending toward the ileocecal junction within the small intestine mesentery (arrows). C Coronal CT image shows a heterogeneous mass (white arrows) around the inferior vena cava and aorta. Mass extends superiorly, through the aortic hiatus, to the posterior mediastinum (black arrowheads). The mass also extended into the root of the small bowel mesentery (not shown) along the superior mesenteric artery.
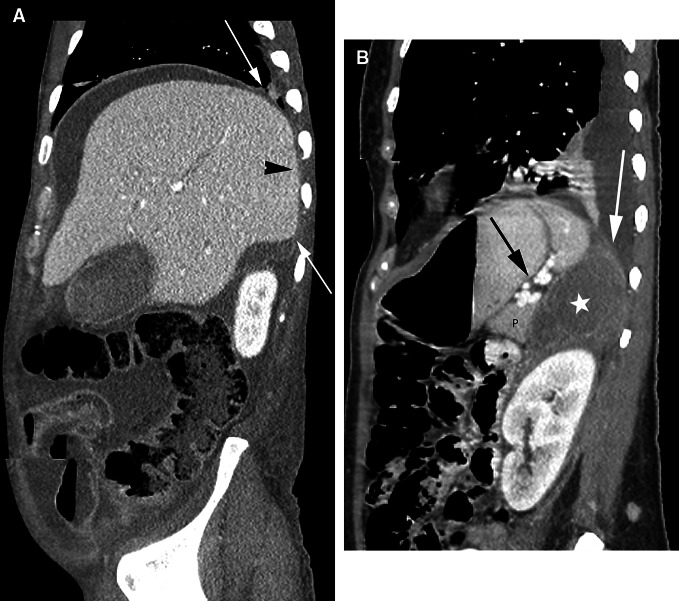
Extraperitoneal spaces in the upper abdomen. A Sagittal CT image shows the peritoneal reflections over the liver (arrows). The liver posterior and medial to these reflections is left bare of peritoneum and abuts the diaphragm (arrowhead). Note that peritoneal fluid surrounds the liver except for the bare area. B Sagittal CT image shows fluid in the left perinephric space (asterisk) extending superiorly to abut the diaphragm (white arrow). The fluid is posterior to the pancreas (P) and the splenorenal ligament (black arrow).
References
-
- Meyers MA, Charnsangavej C, Oliphant M. Meyers’ dynamic radiology of the abdomen: normal and pathologic anatomy. 6. Berlin: Springer Science + Business Media, LLC; 2011.
-
- Standring S, Ellis H, Berkovitz BKB. Gray’s anatomy: the anatomical basis of clinical practice. 39. Amsterdam: Elsevier Churchill Livingstone; 2005.
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
