

Descriptive epidemiology of World Health Organization grades II and III intracranial meningiomas in the United States
- PMID: 26008603
- PMCID: PMC4490879
- DOI: 10.1093/neuonc/nov069
Descriptive epidemiology of World Health Organization grades II and III intracranial meningiomas in the United States
Abstract
Background: Because World Health Organization (WHO) grades II and III meningiomas are relatively uncommon, there is limited literature on the descriptive epidemiology of these tumors, and the existing literature predates the 2000 WHO classification revisions. Our purpose was to provide a modern, population-based study of the descriptive epidemiology of WHO II and III meningiomas in the United States.
Methods: The Central Brain Tumor Registry of the United States (CBTRUS) was queried for intracranial meningiomas categorized by WHO grade for the 2004--2010 study period. Age-adjusted incidence (95% confidence interval in parentheses) per 100,000 population was calculated by age, sex, race, and ethnicity. Annual percent change (APC) was calculated using Joinpoint.
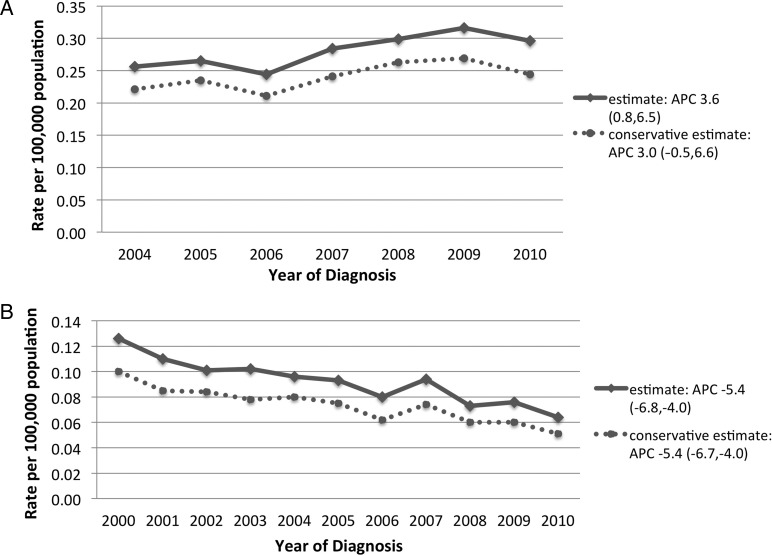
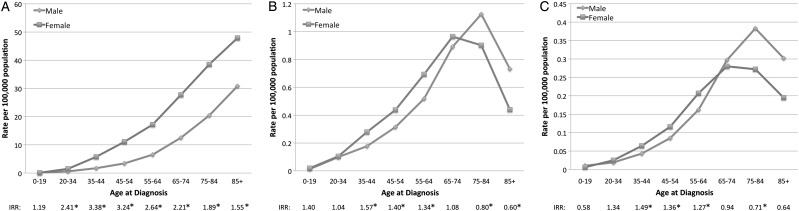
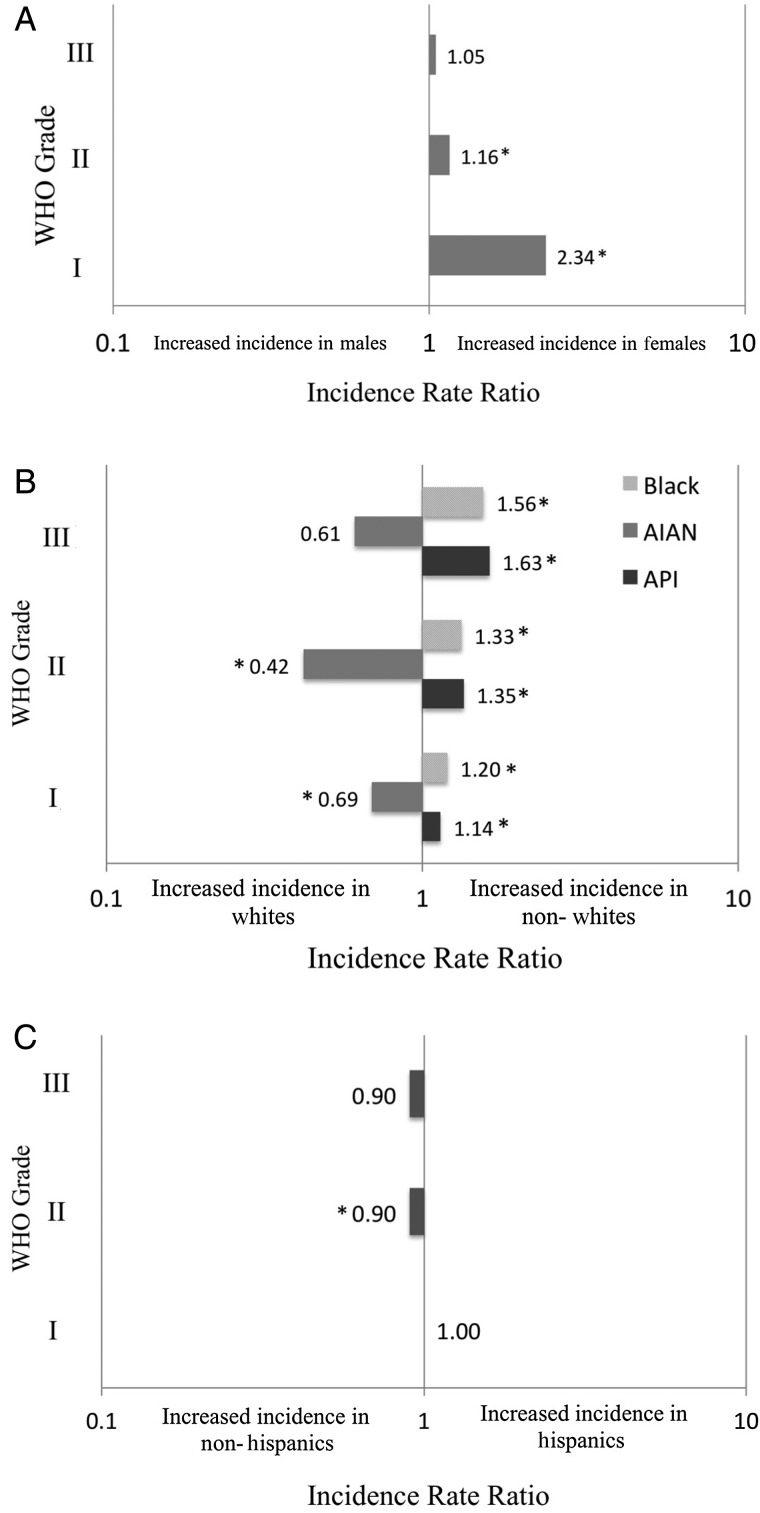
Results: From 2004 to 2010, the incidence of WHO II intracranial meningiomas increased from 0.28 (95% CI, 0.27--0.29) to 0.30 (95% CI, 0.28-0.32), representing an APC of 3.6% (95%CI, 0.8%-6.5%). Conversely, from 2000-2010, the incidence of WHO III meningiomas decreased from 0.13 (95% CI, 0.11-0.14) to 0.06 (95%CI, 0.06-0.07), representing an APC of -5.4% (95% CI, -6.8% to -4.0%). From 2004 to 2010, the overall proportion of WHO I, II, and III intracranial meningiomas was 94.6%, 4.2%, and 1.2%, respectively. For WHO II/III meningiomas, females in the 35-64 year age group had a higher incidence than males in the same age group, whereas males in the ≥ 75 year age group ≥ had a higher incidence. Black and Asian Pacific Islander races were both associated with the highest incidence of WHO II/III meningiomas. Hispanic ethnicity was not associated with any difference in incidence.
Conclusion: This study presents the most comprehensive evaluation of the modern descriptive epidemiology of WHO II and III meningiomas. Temporal trends likely reflect the 2000 WHO histological criteria revisions.
Keywords: anaplastic; atypical; epidemiology; malignant; meningioma.
© The Author(s) 2015. Published by Oxford University Press on behalf of the Society for Neuro-Oncology. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com.
Figures
References
-
- Claus EB, Bondy ML, Schildkraut JM, et al. Epidemiology of intracranial meningioma. Neurosurgery. 2005;57(6):1088–1095. discussion 1088–1095. - PubMed
-
- Combs SE, Schulz-Ertner D, Debus J, et al. Improved correlation of the neuropathologic classification according to adapted world health organization classification and outcome after radiotherapy in patients with atypical and anaplastic meningiomas. Int J Radiat Oncol Biol Phys. 2011;81(5):1415–1421. - PubMed
-
- Krayenbuhl N, Pravdenkova S, Al-Mefty O. De novo versus transformed atypical and anaplastic meningiomas: comparisons of clinical course, cytogenetics, cytokinetics, and outcome. Neurosurgery. 2007;61(3):495–503, discussion 503–494. - PubMed
-
- Modha A, Gutin PH. Diagnosis and treatment of atypical and anaplastic meningiomas: a review. Neurosurgery. 2005;57(3):538–550. discussion 538–550. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
