

Preventing postoperative delirium
- PMID: 26008890
- PMCID: PMC4452898
- DOI: 10.3238/arztebl.2015.0289
Preventing postoperative delirium
Abstract
Background: Delirium is a common complication in elderly hospitalized patients. It prolongs the length of hospital stay, raises costs, increases the workload of the nursing staff, and may necessitate transfer of the patient to a nursing home. The risk of postoperative delirium is particularly high in elderly patients with pre-existing cognitive deficits.
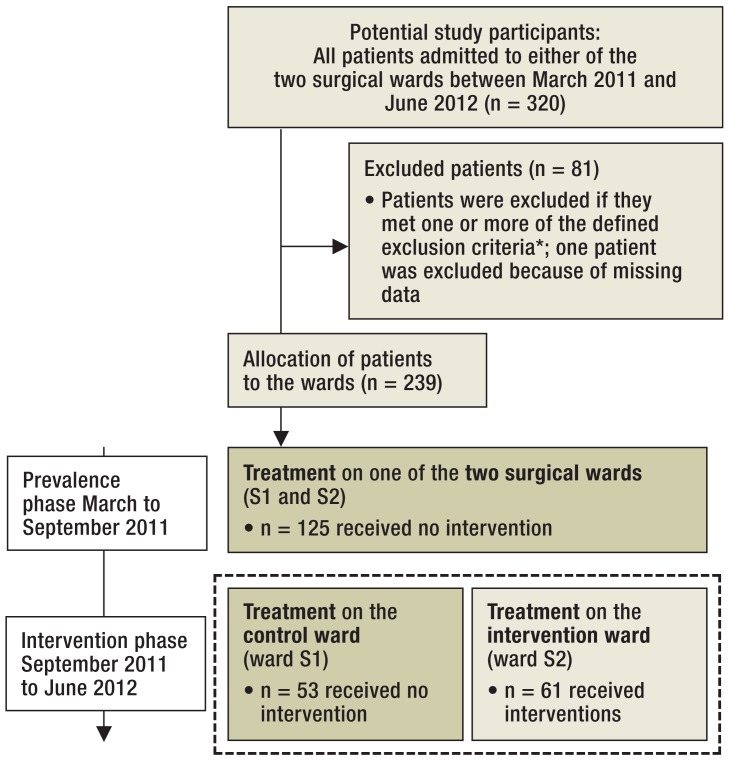
Methods: In an open study, we systematically assessed the frequency of postoperative delirium in patients over age 70 on two surgical wards of a general hospital. In a six-month "prevalence phase," from March to August 2011, we counted the number of patients with postoperative delirium, but did not initiate any intervention. Thereafter, in a ten-month "intervention phase" from September 2011 to June 2012, a nurse with special training in the management of delirium carried out an intervention involving component measures of the Hospital Elder Life Program (HELP) on one of the two wards, with the aim of preventing postoperative delirium. The patients on the other ward served as a control group.
Results: In the prevalence phase, 20.2% of all patients developed postoperative delirium (95% confidence interval [CI], 14.6-26.4). In the intervention phase, postoperative delirium arose in 20.8% (95% CI, 11.3-32.1) of the patients on the ward with no specific interventions, but in only 4.9% (95% CI, 0.0-11.5) of those on the ward where the intervention was carried out. The difference was presumably due to the measures initiated by the specially trained nurse, including validation, improvement of sleep, cognitive activation, early mobilization, improved sensory stimulation, and improved nutritional and fluid intake. Important predictors of postoperative delirium included a low score on the Mini-Mental State Examination, advanced age, and preoperative infection.
Conclusion: The frequency of postoperative delirium in elderly patients with cognitive deficits can be lowered with nursing measures carried out by a specially trained nurse, close postoperative supervision, and cognitive activation.
Figures
Comment in
-
Reproducible Success.Dtsch Arztebl Int. 2015 Oct 9;112(41):692. doi: 10.3238/arztebl.2015.0692a. Dtsch Arztebl Int. 2015. PMID: 26554317 Free PMC article. No abstract available.
-
In Reply.Dtsch Arztebl Int. 2015 Oct 9;112(41):692. doi: 10.3238/arztebl.2015.0692b. Dtsch Arztebl Int. 2015. PMID: 26554318 Free PMC article. No abstract available.
Similar articles
-
A nurse-led interdisciplinary intervention program for delirium in elderly hip-fracture patients.J Am Geriatr Soc. 2001 May;49(5):523-32. doi: 10.1046/j.1532-5415.2001.49109.x. J Am Geriatr Soc. 2001. PMID: 11380743 Clinical Trial.
-
Outcomes of a Geriatric Liaison Intervention to Prevent the Development of Postoperative Delirium in Frail Elderly Cancer Patients: Report on a Multicentre, Randomized, Controlled Trial.PLoS One. 2013 Jun 19;8(6):e64834. doi: 10.1371/journal.pone.0064834. Print 2013. PLoS One. 2013. PMID: 23840308 Free PMC article. Clinical Trial.
-
Postoperative delirium is an independent risk factor for posttraumatic stress disorder in the elderly patient: a prospective observational study.Eur J Anaesthesiol. 2015 Mar;32(3):147-51. doi: 10.1097/EJA.0000000000000107. Eur J Anaesthesiol. 2015. PMID: 24979586
-
[Postoperative cognitive dysfunction of older surgical patients].Medicina (Kaunas). 2010;46(3):169-75. Medicina (Kaunas). 2010. PMID: 20516755 Review. Lithuanian.
-
Delirium and the older adult after surgery.Perspectives. 2004 Spring;28(1):10-6. Perspectives. 2004. PMID: 15315205 Review.
Cited by
-
Preoperative Risk Factors Associated with Increased Incidence of Postoperative Delirium: Systematic Review of Qualified Clinical Studies.Geriatrics (Basel). 2023 Feb 7;8(1):24. doi: 10.3390/geriatrics8010024. Geriatrics (Basel). 2023. PMID: 36826366 Free PMC article. Review.
-
Postoperative Complications Associated With Spine Surgery in Patients Older Than 90 Years: A Multicenter Retrospective Study.Global Spine J. 2018 Dec;8(8):887-891. doi: 10.1177/2192568218767430. Epub 2018 Apr 19. Global Spine J. 2018. PMID: 30560042 Free PMC article. Review.
-
[Competence, creativity and communication: basics for quality improvement in traumatology : Reality and future challenges].Chirurg. 2021 Mar;92(3):210-216. doi: 10.1007/s00104-020-01347-9. Epub 2021 Jan 29. Chirurg. 2021. PMID: 33512560 Free PMC article. Review. German.
-
The Effect of Multidimensional Nursing Interventions on the Incidence of Delirium in Patients with COVID-19.Iran J Nurs Midwifery Res. 2024 Nov 20;29(6):714-719. doi: 10.4103/ijnmr.ijnmr_59_23. eCollection 2024 Nov-Dec. Iran J Nurs Midwifery Res. 2024. PMID: 39759907 Free PMC article.
-
[Frailty as potential indicator of perioperative risk for older patients].Anaesthesist. 2020 Mar;69(3):151-158. doi: 10.1007/s00101-019-00699-0. Anaesthesist. 2020. PMID: 31802172 Review. German.
References
-
- Dilling H, Mombour W, Schmidt MH. Klinisch-diagnostische Leitlinien nach Kapitel V (F) der ICD-10. 9th edition. Bern: Huber Verlag; 2014. Klassifikation psychischer Krankheiten.
-
- Saß H, Wittchen H, Zaudig M. Göttingen: Hogrefe Verlag; 2000. Diagnostisches und Statistisches Manual psychiatrischer Störungen DSM-IV 3rd edition.
-
- Bickel H, Gradinger R, Kochs E, Förstl H. High risk of cognitive and functional decline after postoperative delirium: a three year prospective study. Dement Geriatr Cogn Disord. 2008;26:26–31. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical