

Residual Cardiovascular Risk in Chronic Kidney Disease: Role of High-density Lipoprotein
- PMID: 26009251
- PMCID: PMC4805367
- DOI: 10.1016/j.arcmed.2015.05.009
Residual Cardiovascular Risk in Chronic Kidney Disease: Role of High-density Lipoprotein
Abstract
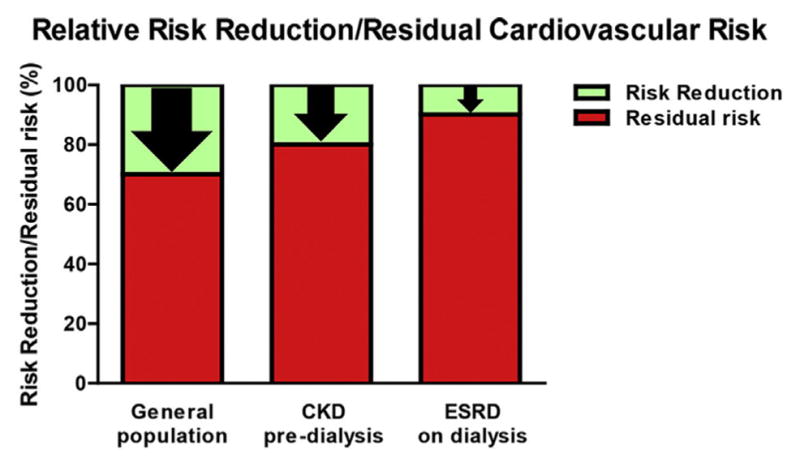
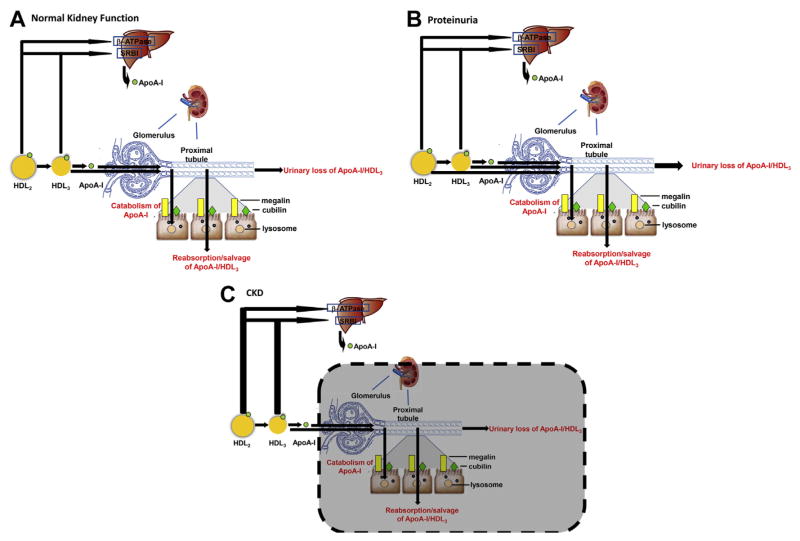
Although reducing low-density lipoprotein-cholesterol (LDL-C) levels with lipid-lowering agents (statins) decreases cardiovascular disease (CVD) risk, a substantial residual risk (up to 70% of baseline) remains after treatment in most patient populations. High-density lipoprotein (HDL) is a potential contributor to residual risk, and low HDL-cholesterol (HDL-C) is an established risk factor for CVD. However, in contrast to conventional lipid-lowering therapies, recent studies show that pharmacologic increases in HDL-C levels do not bring about clinical benefits. These observations have given rise to the concept of dysfunctional HDL where increases in serum HDL-C may not be beneficial because HDL loss of function is not corrected by or even intensified by the therapy. Chronic kidney disease (CKD) increases CVD risk, and patients whose CKD progresses to end-stage renal disease (ESRD) requiring dialysis are at the highest CVD risk of any patient type studied. The ESRD population is also unique in its lack of significant benefit from standard lipid-lowering interventions. Recent studies indicate that HDL-C levels do not predict CVD in the CKD population. Moreover, CKD profoundly alters metabolism and composition of HDL particles and impairs their protective effects on functions such as cellular cholesterol efflux, endothelial protection, and control of inflammation and oxidation. Thus, CKD-induced perturbations in HDL may contribute to the excess CVD in CKD patients. Understanding the mechanisms of vascular protection in renal disease can present new therapeutic targets for intervention in this population.
Keywords: Cardiovascular disease; Cholesterol efflux; Chronic kidney disease; HDL; Residual cardiovascular risk; Statins.
Copyright © 2015 IMSS. Published by Elsevier Inc. All rights reserved.
Figures
Similar articles
-
Importance of high-density lipoprotein quality: evidence from chronic kidney disease.Curr Opin Nephrol Hypertens. 2013 May;22(3):259-65. doi: 10.1097/MNH.0b013e32835fe47f. Curr Opin Nephrol Hypertens. 2013. PMID: 23470818 Free PMC article. Review.
-
Lipid-modifying therapy in chronic kidney disease: Pathophysiological and clinical considerations.Pharmacol Ther. 2020 Mar;207:107459. doi: 10.1016/j.pharmthera.2019.107459. Epub 2019 Dec 18. Pharmacol Ther. 2020. PMID: 31863818 Review.
-
Reasons for the lack of salutary effects of cholesterol-lowering interventions in end-stage renal disease populations.Blood Purif. 2013;35(1-3):31-6. doi: 10.1159/000345176. Epub 2013 Jan 22. Blood Purif. 2013. PMID: 23343544 Free PMC article. Review.
-
Residual dyslipidemia according to low-density lipoprotein cholesterol, non-high-density lipoprotein cholesterol, and apolipoprotein B among statin-treated US adults: National Health and Nutrition Examination Survey 2009-2010.J Clin Lipidol. 2015 Jul-Aug;9(4):525-32. doi: 10.1016/j.jacl.2015.05.003. Epub 2015 May 16. J Clin Lipidol. 2015. PMID: 26228670
-
Clinical assessment and management of dyslipidemia in patients with chronic kidney disease.Clin Exp Nephrol. 2012 Aug;16(4):522-9. doi: 10.1007/s10157-012-0655-x. Epub 2012 Jun 22. Clin Exp Nephrol. 2012. PMID: 22722878 Review.
Cited by
-
There is urgent need to treat atherosclerotic cardiovascular disease risk earlier, more intensively, and with greater precision: A review of current practice and recommendations for improved effectiveness.Am J Prev Cardiol. 2022 Aug 6;12:100371. doi: 10.1016/j.ajpc.2022.100371. eCollection 2022 Dec. Am J Prev Cardiol. 2022. PMID: 36124049 Free PMC article. Review.
-
Association Between Serum High-Density Lipoprotein Cholesterol Levels and Progression of Chronic Kidney Disease: Results From the KNOW-CKD.J Am Heart Assoc. 2019 Mar 19;8(6):e011162. doi: 10.1161/JAHA.118.011162. J Am Heart Assoc. 2019. PMID: 30859896 Free PMC article.
-
Effect of low high-density lipoprotein levels on mortality of septic patients: A systematic review and meta-analysis of cohort studies.World J Emerg Med. 2020;11(2):109-116. doi: 10.5847/wjem.j.1920-8642.2020.02.008. World J Emerg Med. 2020. PMID: 32076477 Free PMC article.
-
High-Density Lipoprotein Lipidomics in Chronic Kidney Disease.Clin Chem. 2023 Mar 1;69(3):273-282. doi: 10.1093/clinchem/hvac216. Clin Chem. 2023. PMID: 36644946 Free PMC article.
-
Advanced lipoprotein parameters could better explain atheromatosis in non-diabetic chronic kidney disease patients.Clin Kidney J. 2021 Jul 6;14(12):2591-2599. doi: 10.1093/ckj/sfab113. eCollection 2021 Dec. Clin Kidney J. 2021. PMID: 34950470 Free PMC article.
References
-
- Antman EM, Anbe DT, Armstrong PW, et al. ACC/AHA guidelines for the management of patients with ST-elevation myocardial infarction–executive summary: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the 1999 Guidelines for the Management of Patients With Acute Myocardial Infarction) Circulation. 2004;110:588–636. - PubMed
-
- Briasoulis A, Bakris GL. Chronic kidney disease as a coronary artery disease risk equivalent. Curr Cardiol Rep. 2013;15:340. - PubMed
-
- Go AS, Chertow GM, Fan D, et al. Chronic kidney disease and the risks of death, cardiovascular events, and hospitalization. N Engl J Med. 2004;351:1296–1305. - PubMed
-
- Tonelli M, Wiebe N, Culleton B, et al. Chronic kidney disease and mortality risk: a systematic review. J Am Soc Nephrol. 2006;17:2034–2047. - PubMed
-
- Wright RS, Reeder GS, Herzog CA, et al. Acute myocardial infarction and renal dysfunction: a high-risk combination. Ann Intern Med. 2002;137:563–570. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
