

Oestrogen enhances cardiotoxicity induced by Sunitinib by regulation of drug transport and metabolism
- PMID: 26009590
- PMCID: PMC4560048
- DOI: 10.1093/cvr/cvv152
Oestrogen enhances cardiotoxicity induced by Sunitinib by regulation of drug transport and metabolism
Abstract
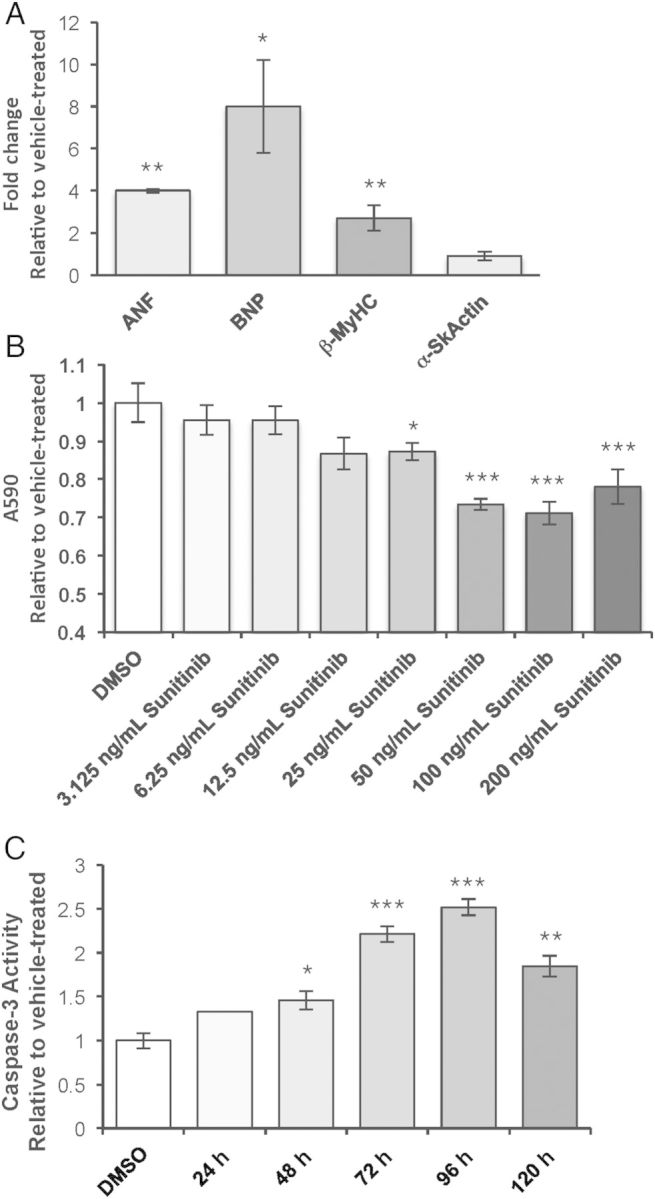
Aims: To define the molecular mechanisms of cardiotoxicity induced by Sunitinib and to identify the role of biological sex in modulating toxicity.
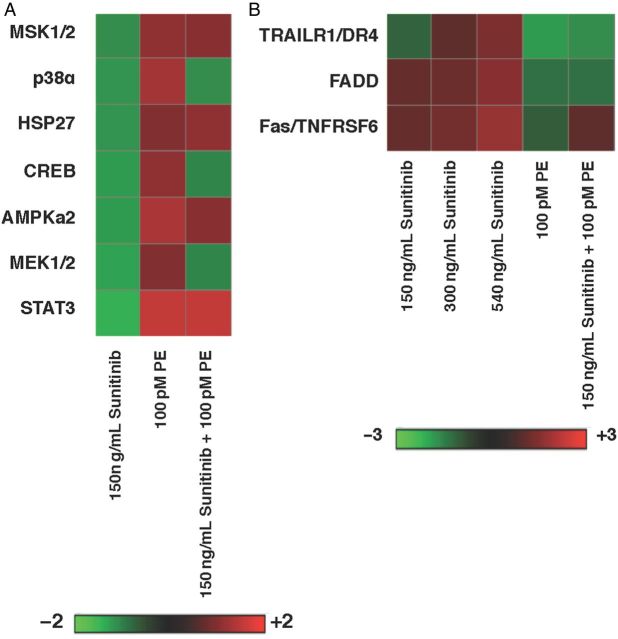
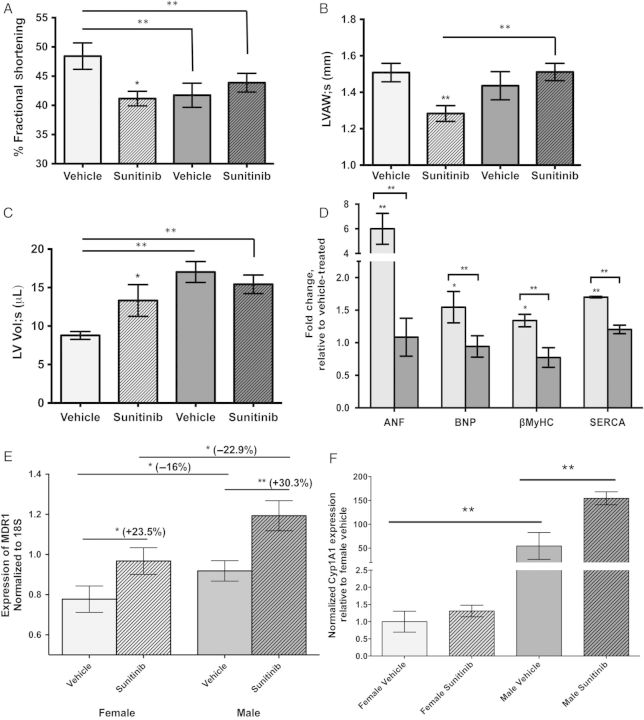
Methods and results: Exposure of isolated cardiomyocytes to plasma-relevant concentrations of Sunitinib and other tyrosine kinase inhibitors produces a broad spectrum of abnormalities and cell death via apoptosis downstream of sexually dimorphic kinase inhibition. Phosphorylation of protein kinase C and phospholipase γ abrogates these effects for most tyrosine kinase inhibitors tested. Female sex and estradiol cause increased cardiotoxicity, which is mediated by reduced expression of a drug efflux transporter and a metabolic enzyme. Female but not male mice exposed to a 28-day course of oral Sunitinib exhibit similar abnormalities as well as functional deficits and their hearts exhibit differential expression of genes responsible for transport and metabolism of Sunitinib.
Conclusion: We identify the specific pathways affected by tyrosine kinase inhibitors in mammalian cardiomyocytes, interactions with biological sex, and a role for oestrogen in modulating drug efflux and metabolism. These findings represent a critical step toward reducing the incidence of cardiotoxicity with tyrosine kinase inhibitor chemotherapeutics.
Keywords: Cardiotoxicity; Cytochrome P450; Multidrug-resistance-1; Oestrogen; Sunitinib.
Published on behalf of the European Society of Cardiology. All rights reserved. © The Author 2015. For permissions please email: journals.permissions@oup.com.
Figures




References
-
- Zhang J, Yang PL, Gray NS. Targeting cancer with small molecule kinase inhibitors. Nat Rev Cancer 2009;9:28–39. - PubMed
-
- Chu TF, Rupnick MA, Kerkela R, Dallabrida SM, Zurakowski D, Nguyen L, Woulfe K, Pravda E, Cassiola F, Desai J, George S, Morgan JA, Harris DM, Ismail NS, Chen JH, Schoen FJ, Van den Abbeele AD, Demetri GD, Force T, Chen MH. Cardiotoxicity associated with tyrosine kinase inhibitor sunitinib. Lancet 2007;370:2011–2019. - PMC - PubMed
-
- Hall PH, Harshman LC, Srinivas S, Witteless RM. The frequency and severity of cardiovascular toxicity from targeted therapy in advanced renal cell carcinoma patients. JACC Heart Failure 2013;1:72–78. - PubMed
-
- Telli ML, Witteles RM, Fisher GA, Srinivas S. Cardiotoxicity associated with the cancer therapeutic agent sunitinib malate. Ann Oncol 2008;19:1613–1618. - PubMed
-
- Kerkela R, Grazette L, Yacobi R, Iliescu C, Patten R, Beahm C, Walters B, Shevtsov S, Pesant S, Clubb FJ, Rosenzweig A, Salomon RN, Van Etten RA, Alroy J, Durand JB, Force T. Cardiotoxicity of the cancer therapeutic agent imatinib mesylate. Nat Med 2006;12:908–916. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
