

Metabolomic fingerprint of heart failure with preserved ejection fraction
- PMID: 26010610
- PMCID: PMC4444296
- DOI: 10.1371/journal.pone.0124844
Metabolomic fingerprint of heart failure with preserved ejection fraction
Abstract
Background: Heart failure (HF) with preserved ejection fraction (HFpEF) is increasingly recognized as an important clinical entity. Preclinical studies have shown differences in the pathophysiology between HFpEF and HF with reduced ejection fraction (HFrEF). Therefore, we hypothesized that a systematic metabolomic analysis would reveal a novel metabolomic fingerprint of HFpEF that will help understand its pathophysiology and assist in establishing new biomarkers for its diagnosis.
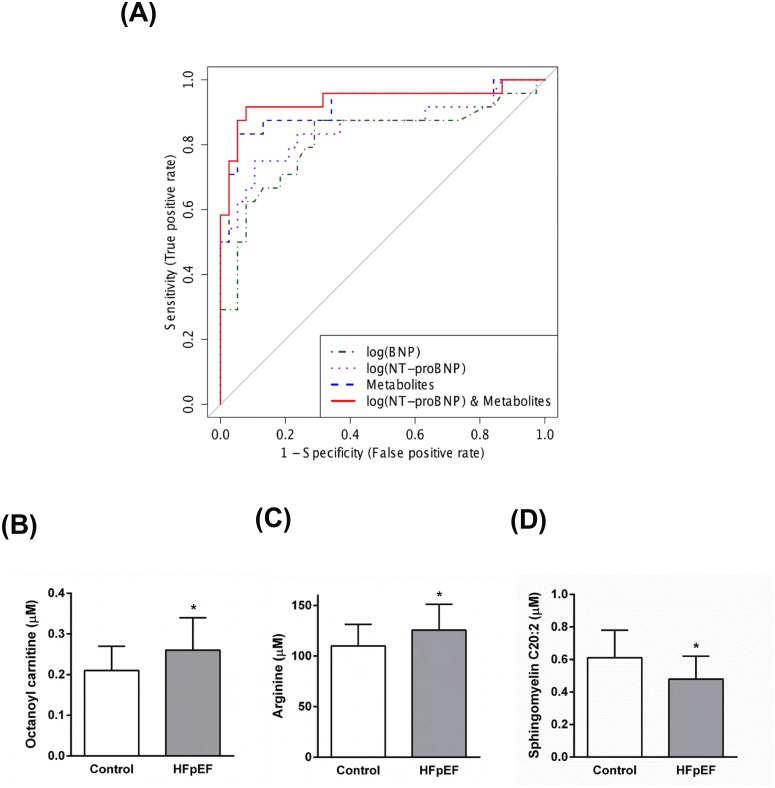
Methods and results: Ambulatory patients with clinical diagnosis of HFpEF (n = 24), HFrEF (n = 20), and age-matched non-HF controls (n = 38) were selected for metabolomic analysis as part of the Alberta HEART (Heart Failure Etiology and Analysis Research Team) project. 181 serum metabolites were quantified by LC-MS/MS and 1H-NMR spectroscopy. Compared to non-HF control, HFpEF patients demonstrated higher serum concentrations of acylcarnitines, carnitine, creatinine, betaine, and amino acids; and lower levels of phosphatidylcholines, lysophosphatidylcholines, and sphingomyelins. Medium and long-chain acylcarnitines and ketone bodies were higher in HFpEF than HFrEF patients. Using logistic regression, two panels of metabolites were identified that can separate HFpEF patients from both non-HF controls and HFrEF patients with area under the receiver operating characteristic (ROC) curves of 0.942 and 0.981, respectively.
Conclusions: The metabolomics approach employed in this study identified a unique metabolomic fingerprint of HFpEF that is distinct from that of HFrEF. This metabolomic fingerprint has been utilized to identify two novel panels of metabolites that can separate HFpEF patients from both non-HF controls and HFrEF patients.
Clinical trial registration: ClinicalTrials.gov NCT02052804.
Conflict of interest statement
Figures







References
-
- Owan TE, Hodge DO, Herges RM, Jacobsen SJ, Roger VL, Redfield MM. Trends in prevalence and outcome of heart failure with preserved ejection fraction. N Engl J Med. 2006;355(3):251–9. - PubMed
-
- Paulus WJ, Tschope C, Sanderson JE, Rusconi C, Flachskampf FA, Rademakers FE, et al. How to diagnose diastolic heart failure: a consensus statement on the diagnosis of heart failure with normal left ventricular ejection fraction by the Heart Failure and Echocardiography Associations of the European Society of Cardiology. Eur Heart J. 2007;28(20):2539–50. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
