

Atypical Antipsychotic Augmentation for Treatment-Resistant Depression: A Systematic Review and Network Meta-Analysis
- PMID: 26012350
- PMCID: PMC4756722
- DOI: 10.1093/ijnp/pyv060
Atypical Antipsychotic Augmentation for Treatment-Resistant Depression: A Systematic Review and Network Meta-Analysis
Abstract
Background: Previous meta-analyses of atypical antipsychotics for depression were limited by few trials with direct comparisons between two treatments. We performed a network meta-analysis, which integrates direct and indirect evidence from randomized controlled trials (RCTs), to investigate the comparative efficacy and tolerability of adjunctive atypical antipsychotics for treatment-resistant depression (TRD).
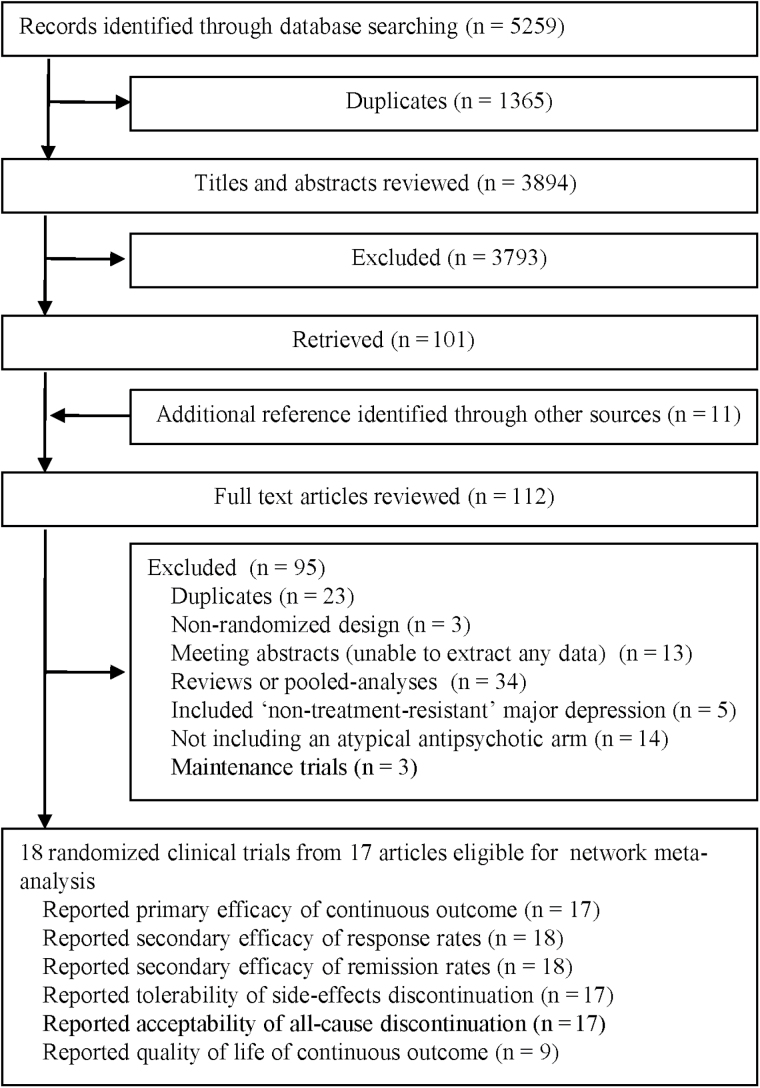
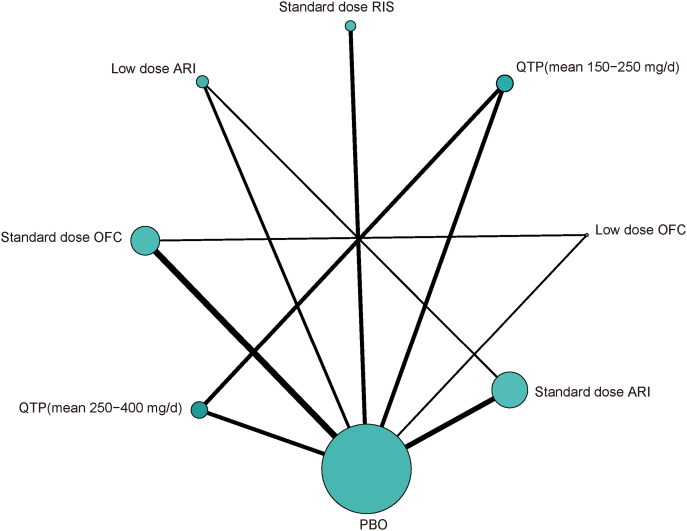
Methods: Systematic searches resulted in 18 RCTs (total n = 4422) of seven different types and different dosages of atypical antipsychotics and a placebo that were included in the review.
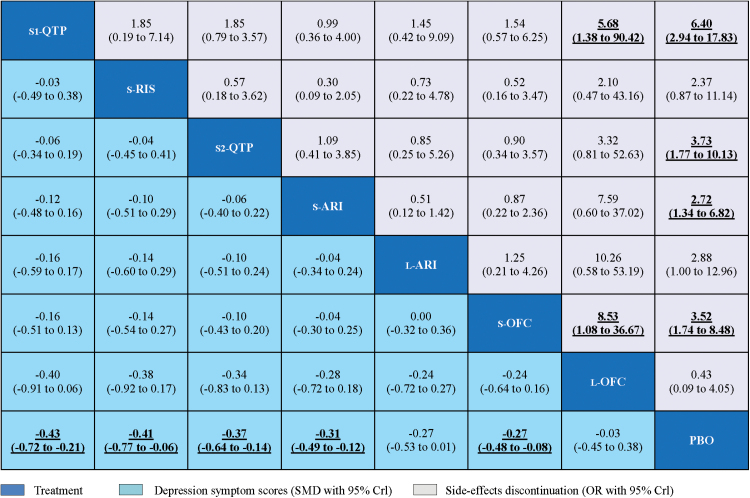
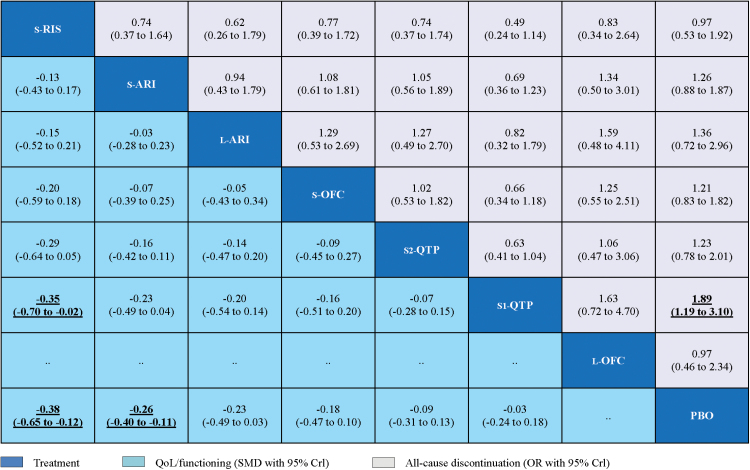
Results: All standard-dose atypical antipsychotics were significantly more efficacious than placebo in the efficacy (standardized mean differences [SMDs] ranged from -0.27 to -0.43). There were no significant differences between these drugs. Low-dose atypical antipsychotics were not significantly more efficacious than the placebo. In terms of tolerability, all standard-dose atypical antipsychotics, apart from risperidone, had significantly more side-effect discontinuations than placebo (odds ratios [ORs] ranged from 2.72 to 6.40). In terms of acceptability, only quetiapine (mean 250-350 mg daily) had significantly more all-cause discontinuation than placebo (OR = 1.89). In terms of quality of life/functioning, standard-dose risperidone and standard-dose aripiprazole were more beneficial than placebo (SMD = -0.38; SMD = -0.26, respectively), and standard-dose risperidone was superior to quetiapine (mean 250-350 mg daily).
Conclusions: All standard-dose atypical antipsychotics for the adjunctive treatment of TRD are efficacious in reducing depressive symptoms. Risperidone and aripiprazole also showed benefits in improving the quality of life of patients. Atypical antipsychotics should be prescribed with caution due to abundant evidence of side effects.
Keywords: Atypical antipsychotics; network meta-analysis; systematic review; treatment-resistant depression.
© The Author 2015. Published by Oxford University Press on behalf of CINP.
Figures
References
-
- Attari A, Moghaddam Y, Hasanzadeh A, Soltani M, Mahmoodi M. (2006) Comparison of efficacy of fluoxetine with nortriptyline in treatment of major depression in children and adolescents: a double-blind study. J Res Med Sci 11:24–30.
-
- Barnes SA, Lindborg SR, Seaman JW. (2006) Multiple imputation techniques in small sample clinical trials. Stat Med 25:233–45. - PubMed
-
- Bauer M, Pretorius HW, Constant EL, Earley WR, Szamosi J, Brecher M. (2009) Extended-release quetiapine as adjunct to an antidepressant in patients with major depressive disorder: results of a randomized, placebo-controlled, double-blind study. J Clin Psychiatry 70:540–549. - PubMed
-
- Bauer M, Pfennig A, Severus E, Whybrow PC, Angst J, Moller HJ, World Federation of Societies of Biological Psychiatry Task Force on Unipolar Depressive D (2013) World Federation of Societies of Biological Psychiatry (WFSBP) guidelines for biological treatment of unipolar depressive disorders, part 1: update 2013 on the acute and continuation treatment of unipolar depressive disorders. World J Biol Psychiatry 14:334–385. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
