

Sedatives and Analgesics Given to Infants in Neonatal Intensive Care Units at the End of Life
- PMID: 26012893
- PMCID: PMC4516679
- DOI: 10.1016/j.jpeds.2015.04.059
Sedatives and Analgesics Given to Infants in Neonatal Intensive Care Units at the End of Life
Abstract
Objective: To describe the administration of sedatives and analgesics at the end of life in a large cohort of infants in North American neonatal intensive care units.
Study design: Data on mortality and sedative and analgesic administration were from infants who died from 1997-2012 in 348 neonatal intensive care units managed by the Pediatrix Medical Group. Sedatives and analgesics of interest included opioids (fentanyl, methadone, morphine), benzodiazepines (clonazepam, diazepam, lorazepam, midazolam), central alpha-2 agonists (clonidine, dexmedetomidine), ketamine, and pentobarbital. We used multivariable logistic regression to evaluate the association between administration of these drugs on the day of death and infant demographics and illness severity.
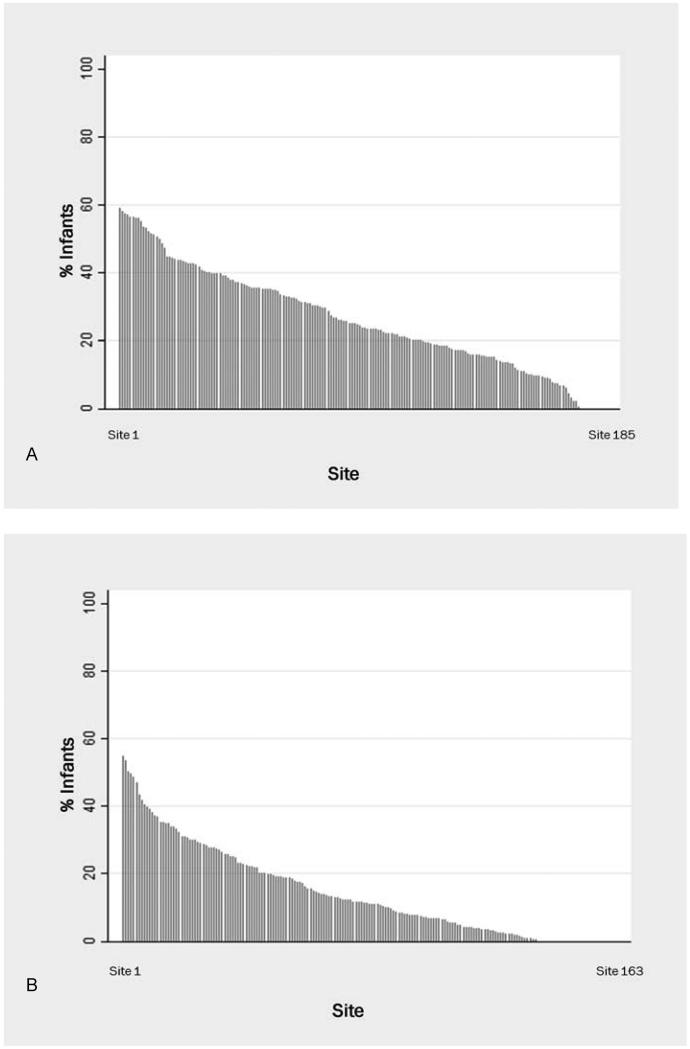
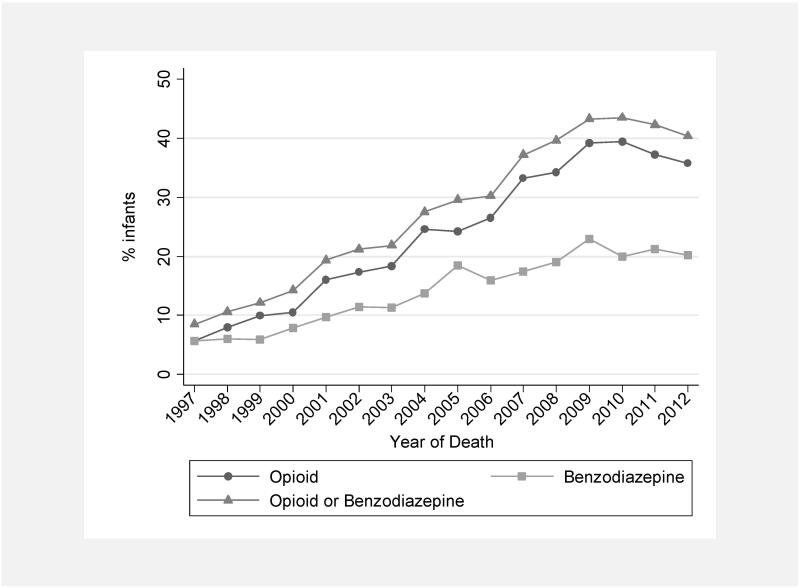
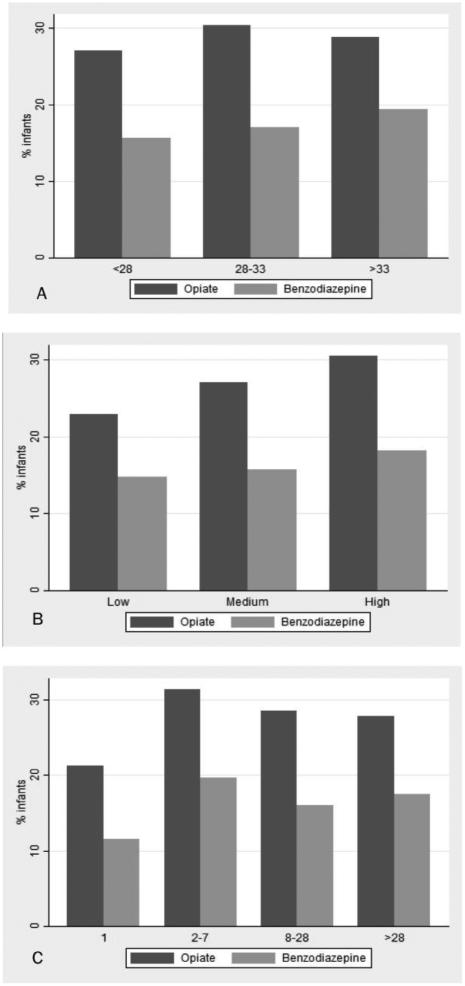
Results: We identified 19 726 infants who died. Of these, 6188 (31%) received a sedative or analgesic on the day of death; opioids were most frequently administered, 5366/19 726 (27%). Administration of opioids and benzodiazepines increased during the study period, from 16/283 (6%) for both in 1997 to 523/1465 (36%) and 295/1465 (20%) in 2012, respectively. Increasing gestational age, increasing postnatal age, invasive procedure within 2 days of death, more recent year of death, mechanical ventilation, inotropic support, and antibiotics on the day of death were associated with exposure to sedatives or analgesics.
Conclusions: Administration of sedatives and analgesics increased over time. Infants of older gestational age and those more critically ill were more likely to receive these drugs on the day of death. These findings suggest that drug administration may be driven by severity of illness.
Copyright © 2015 Elsevier Inc. All rights reserved.
Figures
Similar articles
-
Sedation, Analgesia, and Paralysis during Mechanical Ventilation of Premature Infants.J Pediatr. 2017 Jan;180:99-104.e1. doi: 10.1016/j.jpeds.2016.07.001. Epub 2016 Aug 10. J Pediatr. 2017. PMID: 27522446 Free PMC article.
-
Opioids for newborn infants receiving mechanical ventilation.Cochrane Database Syst Rev. 2021 Mar 17;3(3):CD013732. doi: 10.1002/14651858.CD013732.pub2. Cochrane Database Syst Rev. 2021. PMID: 33729556 Free PMC article.
-
Sedation and analgesia practices at Italian neonatal intensive care units: results from the EUROPAIN study.Ital J Pediatr. 2017 Mar 7;43(1):26. doi: 10.1186/s13052-017-0343-2. Ital J Pediatr. 2017. PMID: 28270167 Free PMC article.
-
Altered Pharmacokinetics in Prolonged Infusions of Sedatives and Analgesics Among Adult Critically Ill Patients: A Systematic Review.Clin Ther. 2018 Sep;40(9):1598-1615.e2. doi: 10.1016/j.clinthera.2018.07.021. Epub 2018 Aug 31. Clin Ther. 2018. PMID: 30173953
-
Oral Feeding Outcome after Analgesic and Sedative Exposure in VLBW Preterm Infant.Am J Perinatol. 2018 Dec;35(14):1399-1404. doi: 10.1055/s-0038-1660468. Epub 2018 Jun 8. Am J Perinatol. 2018. PMID: 29883981
Cited by
-
Sedation, Analgesia, and Paralysis during Mechanical Ventilation of Premature Infants.J Pediatr. 2017 Jan;180:99-104.e1. doi: 10.1016/j.jpeds.2016.07.001. Epub 2016 Aug 10. J Pediatr. 2017. PMID: 27522446 Free PMC article.
-
A qualitative study of nurse observations of symptoms in infants at end-of-life in the neonatal intensive care unit.Intensive Crit Care Nurs. 2017 Jun;40:57-63. doi: 10.1016/j.iccn.2016.10.004. Epub 2017 Feb 8. Intensive Crit Care Nurs. 2017. PMID: 28189383 Free PMC article.
-
Safety of Enalapril in Infants Admitted to the Neonatal Intensive Care Unit.Pediatr Cardiol. 2017 Jan;38(1):155-161. doi: 10.1007/s00246-016-1496-2. Epub 2016 Nov 8. Pediatr Cardiol. 2017. PMID: 27826711 Free PMC article.
-
Emerging Challenges to the Safe and Effective Use of Methadone for Cancer-Related Pain in Paediatric and Adult Patient Populations.Drugs. 2020 Feb;80(2):115-130. doi: 10.1007/s40265-019-01234-6. Drugs. 2020. PMID: 31820362 Review.
-
Creation of a Multicenter Pediatric Inpatient Data Repository Derived from Electronic Health Records.Appl Clin Inform. 2019 Mar;10(2):307-315. doi: 10.1055/s-0039-1688477. Epub 2019 May 8. Appl Clin Inform. 2019. PMID: 31067576 Free PMC article.
References
-
- Rubenfeld GD, Curtis JR. End-of-Life Care in the ICU Working Group. End-of-life care in the intensive care unit: a research agenda. Crit Care Med. 2001;29:2001–6. - PubMed
-
- Truog RD, Campbell ML, Curtis JR, Haas CE, Luce JM, Rubenfeld GD, et al. Recommendations for end-of-life care in the intensive care unit: a consensus statement by the American College [corrected] of Critical Care Medicine. Crit Care Med. 2008;36:953–63. - PubMed
-
- Truog RD, Meyer EC, Burns JP. Toward interventions to improve end-of-life care in the pediatric intensive care unit. Crit Care Med. 2006;34(suppl 11):S373–9. - PubMed
-
- Institute of Medicine . When children die: improving palliative and end-of-life care for children. The National Academies Press; Washington, DC: 2003.
-
- Truog RD, Brock DW, White DB. Should patients receive general anesthesia prior to extubation at the end of life? Crit Care Med. 2012;40:631–3. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
