

High Survivorship With Cementless Stems and Cortical Strut Allografts for Large Femoral Bone Defects in Revision THA
- PMID: 26013152
- PMCID: PMC4523544
- DOI: 10.1007/s11999-015-4358-y
High Survivorship With Cementless Stems and Cortical Strut Allografts for Large Femoral Bone Defects in Revision THA
Abstract
Background: Numerous studies have investigated the clinical and radiographic results of revision THAs with use of cementless stems and cortical strut allografts. However, to our knowledge, no long-term followup studies have evaluated patients undergoing revision THA with use of cortical strut allografts where the allografts provided the primary stability for extensively coated femoral stems in the presence of extensive femoral diaphyseal bone defects.
Question/purposes: We performed this study to determine (1) validated outcomes scores; (2) radiographic signs of fixation and allograft healing; (3) frequency of complications; and (4) survivorship of the components after use of cortical strut onlay allografts in Types IIIB and IV femoral diaphyseal bone defects.
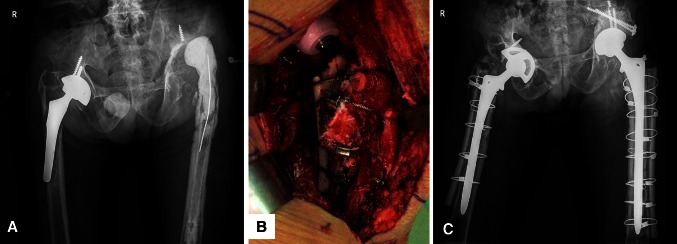
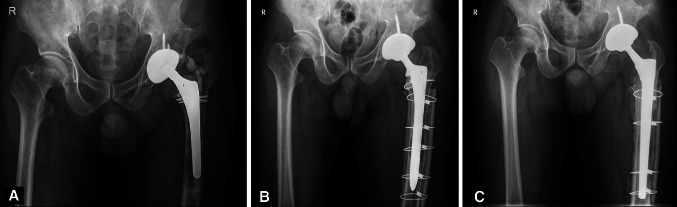
Methods: Between 1994 and 2003, we performed 140 revision THAs in 130 patients with Paprosky Types IIIB and IV femoral diaphyseal defects. The patients were treated using extensively coated femoral stems and cortical strut allografts because primary axial or rotational stability could not be achieved without grafting. Ten of the patients (10 hips; 7.7%) were lost to followup or died before 10 years; the remaining 120 patients (130 hips) represent the study group in this retrospective study. There were 66 men and 54 women. Their mean age at the time of index surgery was 59 ± 18 years (range, 36-67 years). The primary diagnosis was predominantly osteonecrosis of the femoral head (53%). The most common reason for revision was aseptic loosening (97%), followed by periprosthetic fracture (3%). The mean time from primary to revision THA was 12 years (range, 8-27 years). The mean duration of followup was 16.1 years (range, 12-20 years).
Results: The mean Harris hip score was 39 ± 10 points before revision and improved to 86 ± 14 points at 16 years followup (p = 0.02). The mean preoperative WOMAC score was 62 ± 29 (41-91) points and improved to 22 ± 19 (11-51) points at 16 years followup (p = 0.003). Of the 130 stems, 113 (87%) had bone ingrowth, five (4%) had stable fibrous ingrowth, and 12 (9%) were unstable. All allografts were incorporated. Four hips (3%) had a displaced femoral shaft fracture at the stem tip; four (3%) had a postoperative dislocation; and six (5%) had early postoperative infection. Kaplan-Meier survivorship analysis, with revision or radiographic failure as the endpoint, revealed that the 16-year rate of survival of the components was 91% (95% CI, 0.88%-0.96%).
Conclusion: Supportive cortical strut onlay allografts provided high survivorship beyond 12 years of followup in revision THAs. Future studies might compare this approach with allograft-prosthesis composites, proximal femoral replacement, or modular fluted, tapered stems.
Level of evidence: Level IV, therapeutic study.
Figures
Comment in
-
CORR Insights(®): High Survivorship With Cementless Stems and Cortical Strut Allografts for Large Femoral Bone Defects in Revision THA.Clin Orthop Relat Res. 2015 Sep;473(9):3001-2. doi: 10.1007/s11999-015-4399-2. Epub 2015 Jun 13. Clin Orthop Relat Res. 2015. PMID: 26070776 Free PMC article. No abstract available.
Similar articles
-
Long-term results of revision total hip arthroplasties using cementless stems and allografts for paprosky type IIIB and IV femoral defects short title: Revision hip arthroplasty in type IIIB and IV femoral defects.Int Orthop. 2025 Jan;49(1):109-116. doi: 10.1007/s00264-024-06367-2. Epub 2024 Nov 18. Int Orthop. 2025. PMID: 39551896
-
Minimum 8-year follow-up of revision THA with severe femoral bone defects using extensively porous-coated stems and cortical strut allografts.BMC Musculoskelet Disord. 2020 Apr 8;21(1):218. doi: 10.1186/s12891-020-03250-0. BMC Musculoskelet Disord. 2020. PMID: 32268894 Free PMC article.
-
Increased risk of periprosthetic femur fractures associated with a unique cementless stem design.Clin Orthop Relat Res. 2015 Jun;473(6):2045-53. doi: 10.1007/s11999-014-4077-9. Epub 2014 Dec 12. Clin Orthop Relat Res. 2015. PMID: 25502478 Free PMC article.
-
Low Reinfection Rates But a High Rate of Complications in THA for Infection Sequelae in Childhood: A Systematic Review.Clin Orthop Relat Res. 2021 May 1;479(5):1094-1108. doi: 10.1097/CORR.0000000000001607. Clin Orthop Relat Res. 2021. PMID: 33617159 Free PMC article.
-
Long-Term Follow-Up of Management of the Hypoplastic Femur With Femoral Episiotomy and Onlay Allograft During Total Hip Arthroplasty.J Arthroplasty. 2022 Jul;37(7):1308-1313. doi: 10.1016/j.arth.2022.03.028. Epub 2022 Mar 14. J Arthroplasty. 2022. PMID: 35301047 Review.
Cited by
-
Long-term survivorship of a monoblock long cementless stem in revision total hip arthroplasty.Int Orthop. 2019 Oct;43(10):2279-2284. doi: 10.1007/s00264-018-4186-2. Epub 2018 Oct 1. Int Orthop. 2019. PMID: 30276449
-
Long-term results of revision total hip arthroplasties using cementless stems and allografts for paprosky type IIIB and IV femoral defects short title: Revision hip arthroplasty in type IIIB and IV femoral defects.Int Orthop. 2025 Jan;49(1):109-116. doi: 10.1007/s00264-024-06367-2. Epub 2024 Nov 18. Int Orthop. 2025. PMID: 39551896
-
Allogenic bone graft for femoral defect augmentation in hip revision arthroplasty: A case series.Orthop Rev (Pavia). 2020 Apr 28;12(1):8173. doi: 10.4081/or.2020.8173. eCollection 2020 Apr 22. Orthop Rev (Pavia). 2020. PMID: 32391131 Free PMC article.
-
Applications of Carbon Nanotubes in Bone Regenerative Medicine.Nanomaterials (Basel). 2020 Apr 2;10(4):659. doi: 10.3390/nano10040659. Nanomaterials (Basel). 2020. PMID: 32252244 Free PMC article. Review.
-
Femoral revision with primary cementless stems: a systematic review of the literature.Musculoskelet Surg. 2018 Apr;102(1):1-9. doi: 10.1007/s12306-017-0487-7. Epub 2017 Jul 1. Musculoskelet Surg. 2018. PMID: 28669102
References
-
- Bellamy N, Buchanan WW, Goldsmith CH, Campbell J, Stitt LW. Validation study of WOMAC: a health status instrument for measuring clinically important patient relevant outcomes to antirheumatic drug therapy in patients with osteoarthritis of the hip or knee. J Rheumatol. 1988;15:1833–1840. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
