

Response Rates to Anticonvulsant Trials in Patients with Triphasic-Wave EEG Patterns of Uncertain Significance
- PMID: 26013921
- PMCID: PMC4870012
- DOI: 10.1007/s12028-015-0151-8
Response Rates to Anticonvulsant Trials in Patients with Triphasic-Wave EEG Patterns of Uncertain Significance
Abstract
Background: Generalized triphasic waves (TPWs) occur in both metabolic encephalopathies and non-convulsive status epilepticus (NCSE). Empiric trials of benzodiazepines (BZDs) or non-sedating AED (NSAEDs) are commonly used to differentiate the two, but the utility of such trials is debated. The goal of this study was to assess response rates of such trials and investigate whether metabolic profile differences affect the likelihood of a response.
Methods: Three institutions within the Critical Care EEG Monitoring Research Consortium retrospectively identified patients with unexplained encephalopathy and TPWs who had undergone a trial of BZD and/or NSAEDs to differentiate between ictal and non-ictal patterns. We assessed responder rates and compared metabolic profiles of responders and non-responders. Response was defined as resolution of the EEG pattern and either unequivocal improvement in encephalopathy or appearance of previously absent normal EEG patterns, and further categorized as immediate (within <2 h of trial initiation) or delayed (>2 h from trial initiation).
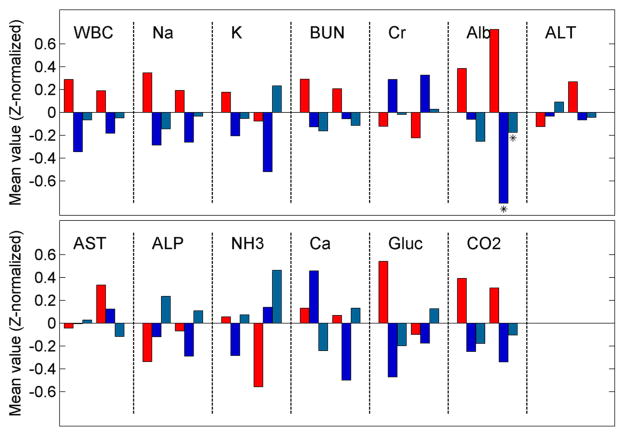
Results: We identified 64 patients with TPWs who had an empiric trial of BZD and/or NSAED. Most patients (71.9%) were admitted with metabolic derangements and/or infection. Positive clinical responses occurred in 10/53 (18.9%) treated with BZDs. Responses to NSAEDs occurred in 19/45 (42.2%), being immediate in 6.7%, delayed but definite in 20.0%, and delayed but equivocal in 15.6%. Overall, 22/64 (34.4%) showed a definite response to either BZDs or NSAEDs, and 7/64 (10.9%) showed a possible response. Metabolic differences of responders versus non-responders were statistically insignificant, except that the 48-h low value of albumin in the BZD responder group was lower than in the non-responder group.
Conclusions: Similar metabolic profiles in patients with encephalopathy and TPWs between responders and non-responders to anticonvulsants suggest that predicting responders a priori is difficult. The high responder rate suggests that empiric trials of anticonvulsants indeed provide useful clinical information. The more than twofold higher response rate to NSAEDs suggests that this strategy may be preferable to BZDs. Further prospective investigation is warranted.
Keywords: Encephalopathy; Generalized periodic discharges; Non-convulsive status epilepticus; Triphasic waves.
Figures
Similar articles
-
Inadequate benzodiazepine dosing may result in progression to refractory and non-convulsive status epilepticus.Epileptic Disord. 2018 Aug 1;20(4):265-269. doi: 10.1684/epd.2018.0987. Epileptic Disord. 2018. PMID: 30113012
-
Ictal and interictal EEG patterns in patients with nonconvulsive and subtle convulsive status epilepticus.Epilepsy Behav. 2015 Aug;49:263-7. doi: 10.1016/j.yebeh.2015.05.011. Epub 2015 Jun 14. Epilepsy Behav. 2015. PMID: 26081674
-
The Clinical Features and Prognosis of Patients With Nonconvulsive Status Epilepticus in the Neurological Intensive Care Unit of a Tertiary Referral Center in Turkey.Clin EEG Neurosci. 2014 Oct;45(4):293-298. doi: 10.1177/1550059413503639. Epub 2013 Nov 28. Clin EEG Neurosci. 2014. PMID: 24293162
-
[Non-convulsive status epilepticus].Rev Neurol. 2003 Oct 16-31;37(8):744-52. Rev Neurol. 2003. PMID: 14593634 Review. Spanish.
-
Status epilepticus and the use of continuous EEG monitoring in the intensive care unit.Continuum (Minneap Minn). 2012 Jun;18(3):560-78. doi: 10.1212/01.CON.0000415428.61277.90. Continuum (Minneap Minn). 2012. PMID: 22810249 Review.
Cited by
-
A novel neural computational model of generalized periodic discharges in acute hepatic encephalopathy.J Comput Neurosci. 2019 Dec;47(2-3):109-124. doi: 10.1007/s10827-019-00727-3. Epub 2019 Sep 11. J Comput Neurosci. 2019. PMID: 31506807 Free PMC article.
-
Hypsarrhythmia and triphasic waves seem to be akin(similar) age-dependent responses of the brain to different insults.J Neurosci Rural Pract. 2024 Jan-Mar;15(1):156-158. doi: 10.25259/JNRP_319_2023. Epub 2023 Oct 24. J Neurosci Rural Pract. 2024. PMID: 38476411 Free PMC article. No abstract available.
-
Clinical analysis of 20 cases of brain injury caused by diabetic ketoacidosis in children.BMC Pediatr. 2025 Jul 23;25(1):566. doi: 10.1186/s12887-025-05927-8. BMC Pediatr. 2025. PMID: 40702455 Free PMC article.
-
Outcomes of seizures, status epilepticus, and EEG findings in critically ill patient with COVID-19.Epilepsy Behav. 2021 May;118:107923. doi: 10.1016/j.yebeh.2021.107923. Epub 2021 Mar 8. Epilepsy Behav. 2021. PMID: 33770609 Free PMC article.
-
Ictal Interictal Continuum Patterns.Curr Treat Options Neurol. 2018 Apr 18;20(5):15. doi: 10.1007/s11940-018-0500-y. Curr Treat Options Neurol. 2018. PMID: 29666958 Review.
References
-
- Bahamon-Dussan JE, Celesia GG, Grigg-Damberger MM. Prognostic significance of EEG triphasic waves in patients with altered state of consciousness. J Clin Neurophysiol Off Publ Am Electroencephalogr Soc. 1989;6:313–9. - PubMed
-
- Eidelman LA, Putterman D, Putterman C, Sprung CL. The spectrum of septic encephalopathy. Definitions, etiologies, and mortalities. JAMA. 1996;275:470–3. - PubMed
-
- Ely EW, Shintani A, Truman B, Speroff T, Gordon SM, Harrell FE, et al. Delirium as a predictor of mortality in mechanically ventilated patients in the intensive care unit. JAMA. 2004;291:1753–62. - PubMed
-
- Ogunyemi A. Triphasic waves during post-ictal stupor. Can J Neurol Sci. 1996;23:208–12. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
