

Feasibility of Large-Scale Genomic Testing to Facilitate Enrollment Onto Genomically Matched Clinical Trials
- PMID: 26014291
- PMCID: PMC4550690
- DOI: 10.1200/JCO.2014.60.4165
Feasibility of Large-Scale Genomic Testing to Facilitate Enrollment Onto Genomically Matched Clinical Trials
Abstract
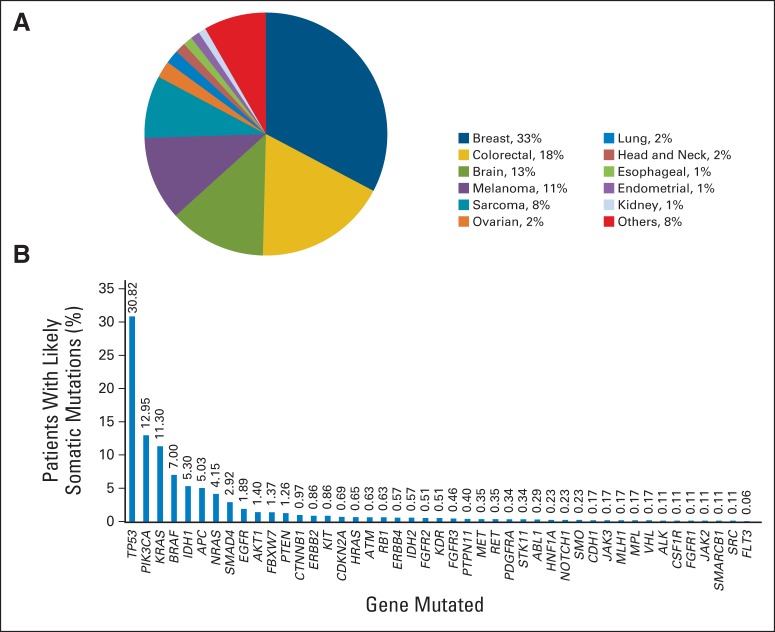
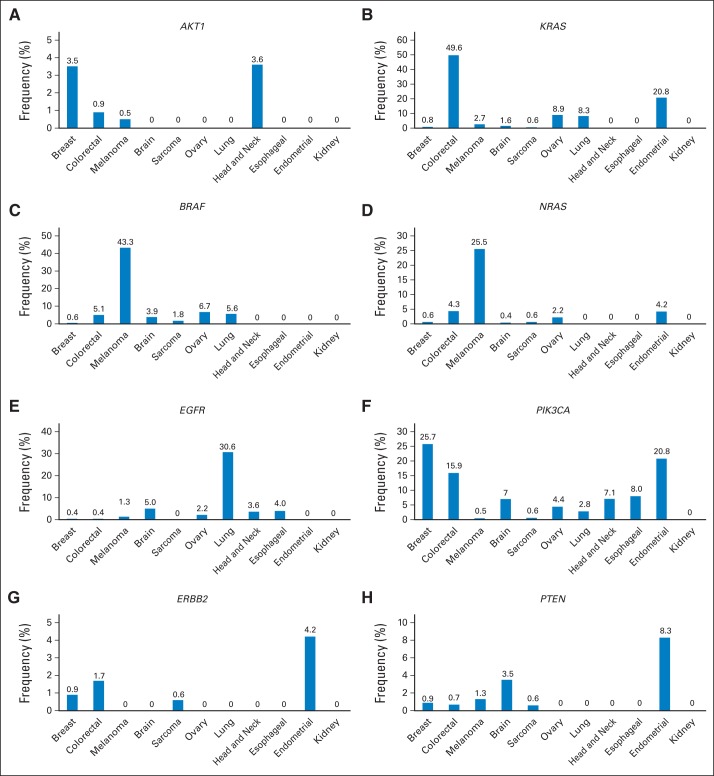
Purpose: We report the experience with 2,000 consecutive patients with advanced cancer who underwent testing on a genomic testing protocol, including the frequency of actionable alterations across tumor types, subsequent enrollment onto clinical trials, and the challenges for trial enrollment.
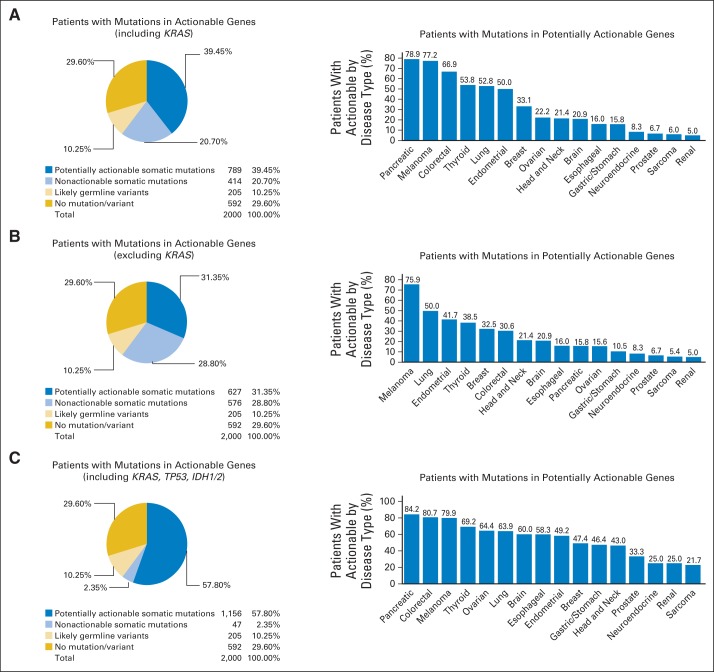
Patients and methods: Standardized hotspot mutation analysis was performed in 2,000 patients, using either an 11-gene (251 patients) or a 46- or 50-gene (1,749 patients) multiplex platform. Thirty-five genes were considered potentially actionable based on their potential to be targeted with approved or investigational therapies.
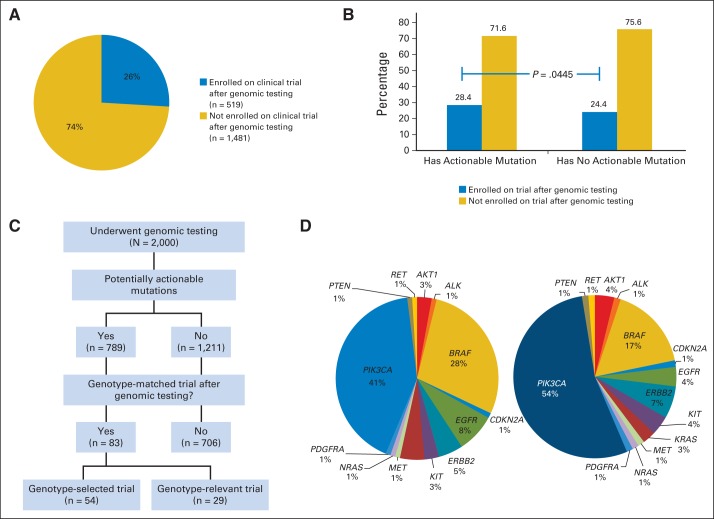
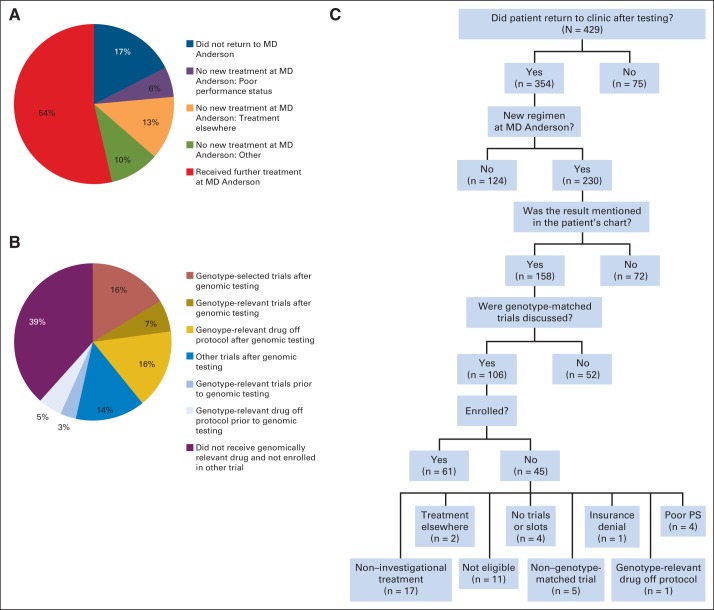
Results: Seven hundred eighty-nine patients (39%) had at least one mutation in potentially actionable genes. Eighty-three patients (11%) with potentially actionable mutations went on genotype-matched trials targeting these alterations. Of 230 patients with PIK3CA/AKT1/PTEN/BRAF mutations that returned for therapy, 116 (50%) received a genotype-matched drug. Forty patients (17%) were treated on a genotype-selected trial requiring a mutation for eligibility, 16 (7%) were treated on a genotype-relevant trial targeting a genomic alteration without biomarker selection, and 40 (17%) received a genotype-relevant drug off trial. Challenges to trial accrual included patient preference of noninvestigational treatment or local treatment, poor performance status or other reasons for trial ineligibility, lack of trials/slots, and insurance denial.
Conclusion: Broad implementation of multiplex hotspot testing is feasible; however, only a small portion of patients with actionable alterations were actually enrolled onto genotype-matched trials. Increased awareness of therapeutic implications and access to novel therapeutics are needed to optimally leverage results from broad-based genomic testing.
© 2015 by American Society of Clinical Oncology.
Conflict of interest statement
Authors' disclosures of potential conflicts of interest are found in the article online at
Figures
Comment in
-
Tumor Genetic Screening Programs: A Call to Action.J Clin Oncol. 2015 Sep 1;33(25):2725-6. doi: 10.1200/JCO.2015.61.9296. Epub 2015 Jul 20. J Clin Oncol. 2015. PMID: 26195721 No abstract available.
-
Enrolling patients into genomically matched clinical trials found challenging.CA Cancer J Clin. 2015 Nov-Dec;65(6):425-6. doi: 10.3322/caac.21316. Epub 2015 Sep 9. CA Cancer J Clin. 2015. PMID: 26352666 No abstract available.
-
Clinician Perspective on Molecular Profiling of Non-Small-Cell Lung Cancer.J Clin Oncol. 2016 Mar 10;34(8):884-6. doi: 10.1200/JCO.2015.65.2040. Epub 2016 Jan 11. J Clin Oncol. 2016. PMID: 26755521 No abstract available.
-
Reply to M.P. Decatris et al.J Clin Oncol. 2016 Mar 10;34(8):886. doi: 10.1200/JCO.2015.65.2479. Epub 2016 Jan 11. J Clin Oncol. 2016. PMID: 26755522 No abstract available.
References
-
- Routbort MJ, Handal BA, Patel KP, et al. OncoSeek: A versatile annotation and reporting system for next generation sequencing-based clinical mutation analysis of cancer specimens. J Mol Diagn. 2012;14:747. (abstr)
-
- Singh RR, Patel KP, Routbort MJ, et al. Clinical validation of a next-generation sequencing screen for mutational hotspots in 46 cancer-related genes. J Mol Diagn. 2013;15:607–622. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
