

Hospitalization Type and Subsequent Severe Sepsis
- PMID: 26016947
- PMCID: PMC4595694
- DOI: 10.1164/rccm.201503-0483OC
Hospitalization Type and Subsequent Severe Sepsis
Abstract
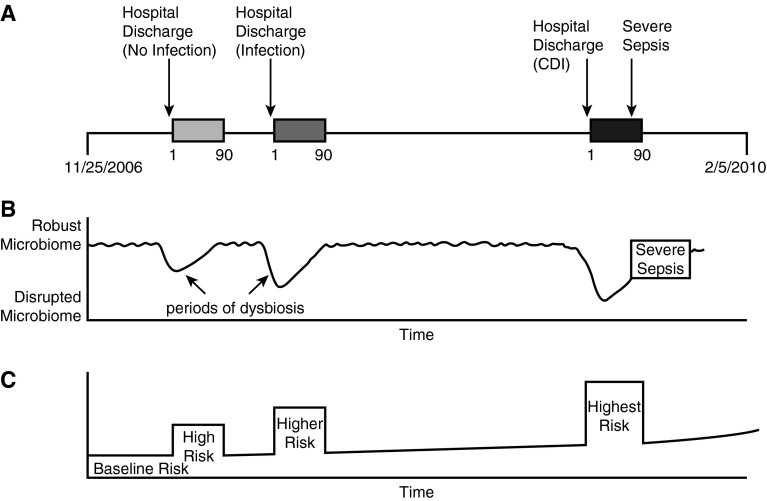
Rationale: Hospitalization is associated with microbiome perturbation (dysbiosis), and this perturbation is more severe in patients treated with antimicrobials.
Objectives: To evaluate whether hospitalizations known to be associated with periods of microbiome perturbation are associated with increased risk of severe sepsis after hospital discharge.
Methods: We studied participants in the U.S. Health and Retirement Study with linked Medicare claims (1998-2010). We measured whether three hospitalization types associated with increasing severity of probable dysbiosis (non-infection-related hospitalization, infection-related hospitalization, and hospitalization with Clostridium difficile infection [CDI]) were associated with increasing risk for severe sepsis in the 90 days after hospital discharge. We used two study designs: the first was a longitudinal design with between-person comparisons and the second was a self-controlled case series design using within-person comparison.
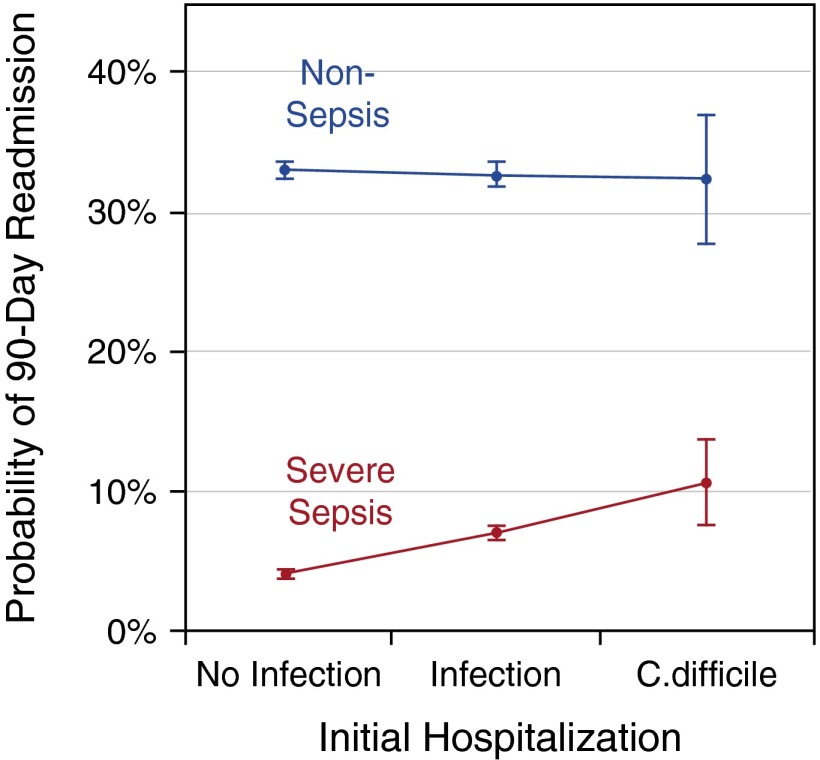
Measurements and main results: We identified 43,095 hospitalizations among 10,996 Health and Retirement Study-Medicare participants. In the 90 days following non-infection-related hospitalization, infection-related hospitalization, and hospitalization with CDI, adjusted probabilities of subsequent admission for severe sepsis were 4.1% (95% confidence interval [CI], 3.8-4.4%), 7.1% (95% CI, 6.6-7.6%), and 10.7% (95% CI, 7.7-13.8%), respectively. The incidence rate ratio (IRR) of severe sepsis was 3.3-fold greater during the 90 days after hospitalizations than during other observation periods. The IRR was 30% greater after an infection-related hospitalization versus a non-infection-related hospitalization. The IRR was 70% greater after a hospitalization with CDI than an infection-related hospitalization without CDI.
Conclusions: There is a strong dose-response relationship between events known to result in dysbiosis and subsequent severe sepsis hospitalization that is not present for rehospitalization for nonsepsis diagnoses.
Keywords: dysbiosis; humans; microbiota; patient readmission; self-controlled case series.
Figures
References
-
- Ley RE, Peterson DA, Gordon JI. Ecological and evolutionary forces shaping microbial diversity in the human intestine. Cell. 2006;124:837–848. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical