

Fibular head transfixion wire and its relationship to common peroneal nerve: cadaveric analysis
- PMID: 26017165
- PMCID: PMC4570888
- DOI: 10.1007/s11751-015-0225-3
Fibular head transfixion wire and its relationship to common peroneal nerve: cadaveric analysis
Abstract
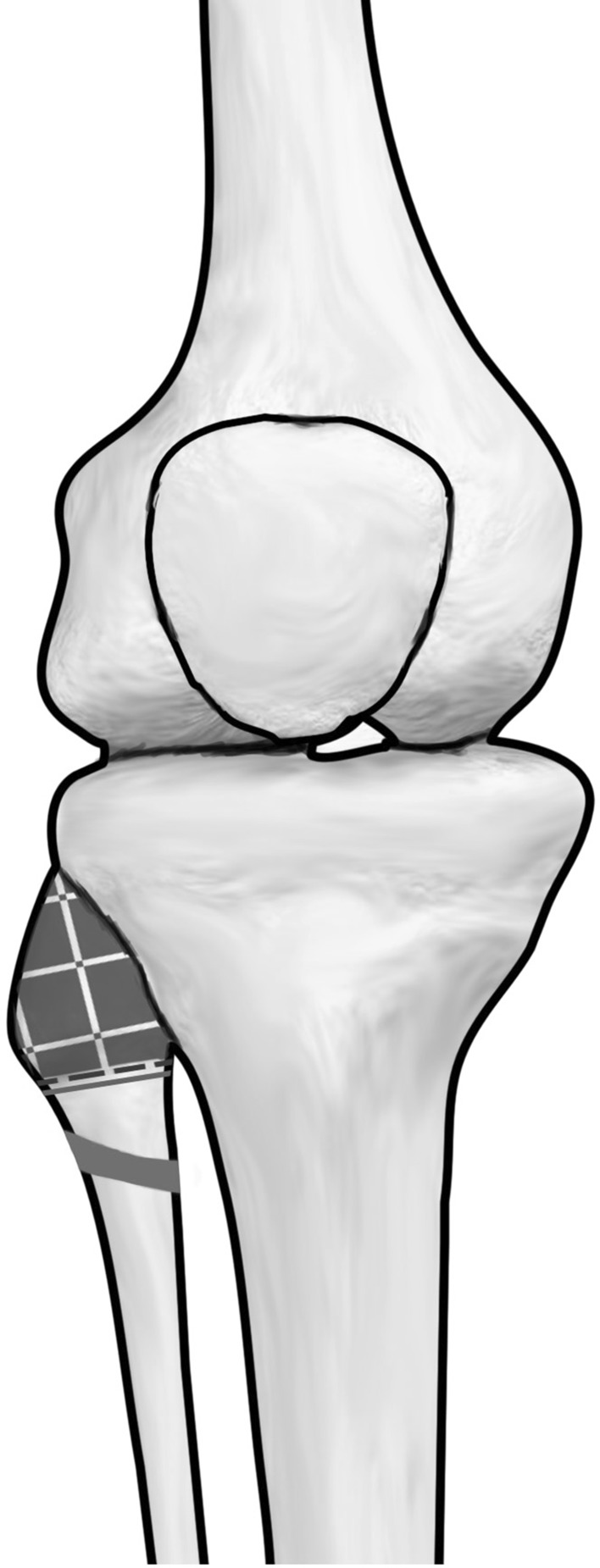
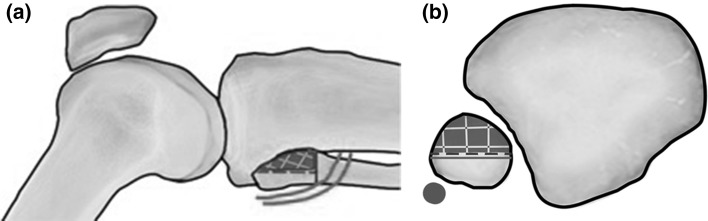
Proximal tibio-fibular joint is routinely stabilised during leg lengthening, peri-articular fractures and deformity corrections of tibia. Potential injury to the common peroneal nerve at the level of the fibula head/neck junction during wire insertion is a recognised complication. Previous studies have mapped the course of the common peroneal nerve and its branches at the level of the fibular head, and guidelines are published regarding placement of proximal tibial wires. This study aims to relate the course of the common peroneal nerve to the placement of a lateral insertion fibula head transfixion wire. Standard 1.8-mm Ilizarov 'olive' wires were inserted in the fibula head of 10 un-embalmed cadaveric knees. Wires were inserted percutaneously to the fibula head using surface anatomy landmarks and palpation technique. The course of the common peroneal nerve was then dissected. Distances from wire entry point to the course of the common peroneal nerve were measured post-wire insertion. The mean distance of the common peroneal nerve from the anterior aspect of the broadest point of the fibular head was 24.5 mm (range 14.2-37.7 mm). Common peroneal nerve was seen to cross the neck of fibula at a mean distance of 34.8 mm from the tip of fibula (range 21.5-44.3 mm). Wire placement was found to be on average, 52 % of the maximal AP diameter of the fibula head and 64 % of the distance from tip of fibula to the point of nerve crossing fibula neck. When inserting a fibula head transfixion wire, care must be taken not to place wire entry point too distal or posterior on the fibula head. Observing a safe zone in the anterior half of the proximal 20 mm of the fibula head would avoid injury to the nerve. In cases where palpation of fibula is difficult due to patient habitus, we recommend consideration of the use of fluoroscopic guidance during wire transfixion of the proximal tibio-fibular articulation to avoid wire insertion too distally and subsequent potential nerve injury.
Keywords: Anatomy; Frame; Ilizarov; Limb lengthening; Peroneal nerve; Proximal tibial fractures.
Figures



References
-
- Kirgis A, Albrecht S. Palsy of the deep peroneal nerve after proximal tibial osteotomy. An anatomical study. J Bone Joint Surg Am. 1992;74(8):1180–1185. - PubMed
-
- Stitgen SH, Cairns ER, Ebraheim NA, Niemann JM, Jackson WT. Anatomic considerations of pin placement in the proximal tibia and its relationship to the peroneal nerve. Clin Orthop Relat Res. 1992;278:134–137. - PubMed
-
- Reebye O. Anatomical and clinical study of the common fibular nerve. Part 1: anatomical study. Surg Radiol Anat. 2004;26:365–370. - PubMed
-
- Moskovich R. Proximal tibial transfixion for skeletal traction. An anatomic study of neurovascular structures. Clin Orthop Relat Res. 1987;214:264–268. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
