

Enhanced surveillance and data feedback loop associated with improved malaria data in Lusaka, Zambia
- PMID: 26017275
- PMCID: PMC4486393
- DOI: 10.1186/s12936-015-0735-y
Enhanced surveillance and data feedback loop associated with improved malaria data in Lusaka, Zambia
Abstract
Background: Accurate and timely malaria data are crucial to monitor the progress towards and attainment of elimination. Lusaka, the capital city of Zambia, has reported very low malaria prevalence in Malaria Indicator Surveys. Issues of low malaria testing rates, high numbers of unconfirmed malaria cases and over consumption of anti-malarials were common at clinics within Lusaka, however. The Government of Zambia (GRZ) and its partners sought to address these issues through an enhanced surveillance and feedback programme at clinic level.
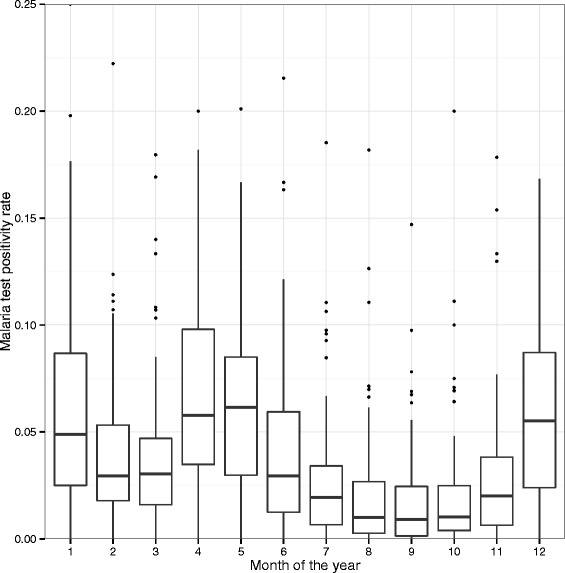
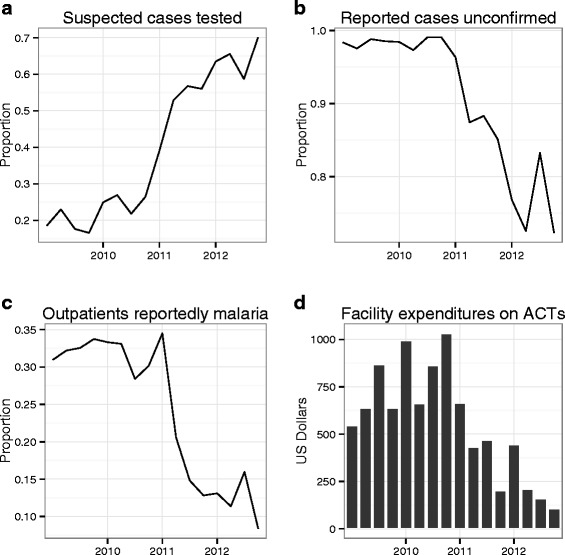
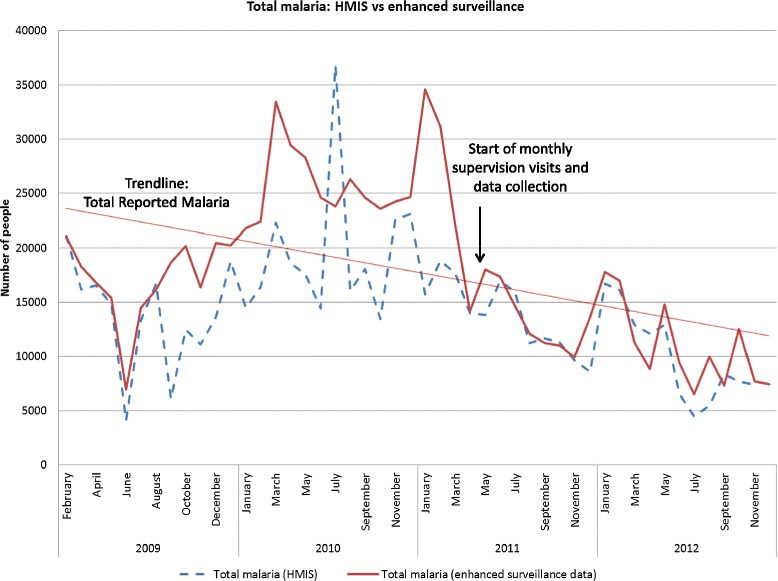
Methods: The enhanced malaria surveillance programme began in 2011 to verify trends in reported malaria, as well as to implement a data feedback loop to improve data uptake, use, and quality. A process of monthly data collection and provision of feedback was implemented within all GRZ health clinics in Lusaka District. During clinic visits, clinic registers were accessed to record the number of reported malaria cases, malaria test positivity rate, malaria testing rate, and proportion of total suspected malaria that was confirmed with a diagnostic test.
Results and discussion: Following the enhanced surveillance programme, the odds of receiving a diagnostic test for a suspected malaria case increased (OR = 1.54, 95 % CI = 0.96-2.49) followed by an upward monthly trend (OR = 1.05, 95 % CI = 1.01-1.09). The odds of a reported malaria case being diagnostically confirmed also increased monthly (1.09, 95 % CI 1.04-1.15). After an initial 140 % increase (95 % CI = 91-183 %), costs fell by 11 % each month (95 % CI = 5.7-10.9 %). Although the mean testing rate increased from 18.9 to 64.4 % over the time period, the proportion of reported malaria unconfirmed by diagnostic remained high at 76 %.
Conclusions: Enhanced surveillance and implementation of a data feedback loop have substantially increased malaria testing rates and decreased the number of unconfirmed malaria cases and courses of ACT consumed in Lusaka District within just two years. Continued support of enhanced surveillance in Lusaka as well as national scale-up of the system is recommended to reinforce good case management and to ensure timely, reliable data are available to guide targeting of limited malaria prevention and control resources in Zambia.
Figures
Similar articles
-
A qualitative review of implementer perceptions of the national community-level malaria surveillance system in Southern Province, Zambia.Malar J. 2016 Aug 8;15(1):400. doi: 10.1186/s12936-016-1455-7. Malar J. 2016. PMID: 27502213 Free PMC article. Review.
-
Malaria surveillance in low-transmission areas of Zambia using reactive case detection.Malar J. 2015 Nov 19;14:465. doi: 10.1186/s12936-015-0895-9. Malar J. 2015. PMID: 26586264 Free PMC article.
-
Human mobility and factors associated with malaria importation in Lusaka district, Zambia: a descriptive cross sectional study.Malar J. 2018 Nov 3;17(1):404. doi: 10.1186/s12936-018-2554-4. Malar J. 2018. PMID: 30390654 Free PMC article.
-
Spatial patterns of incident malaria cases and their household contacts in a single clinic catchment area of Chongwe District, Zambia.Malar J. 2015 Aug 7;14:305. doi: 10.1186/s12936-015-0793-1. Malar J. 2015. PMID: 26246383 Free PMC article.
-
Malaria surveillance counts.Am J Trop Med Hyg. 2007 Dec;77(6 Suppl):36-47. Am J Trop Med Hyg. 2007. PMID: 18165473 Review.
Cited by
-
Trends in reported malaria cases and the effects of malaria control in the Democratic Republic of the Congo.PLoS One. 2019 Jul 25;14(7):e0219853. doi: 10.1371/journal.pone.0219853. eCollection 2019. PLoS One. 2019. PMID: 31344062 Free PMC article.
-
Improvements in malaria surveillance through the electronic Integrated Disease Surveillance and Response (eIDSR) system in mainland Tanzania, 2013-2021.Malar J. 2022 Nov 8;21(1):321. doi: 10.1186/s12936-022-04353-w. Malar J. 2022. PMID: 36348409 Free PMC article.
-
Integrated Disease Surveillance and Response (IDSR) in Malawi: Implementation gaps and challenges for timely alert.PLoS One. 2018 Nov 29;13(11):e0200858. doi: 10.1371/journal.pone.0200858. eCollection 2018. PLoS One. 2018. PMID: 30496177 Free PMC article.
-
Addressing the Disconnect between the Estimated, Reported, and True Rabies Data: The Development of a Regional African Rabies Bulletin.Front Vet Sci. 2017 Feb 20;4:18. doi: 10.3389/fvets.2017.00018. eCollection 2017. Front Vet Sci. 2017. PMID: 28265562 Free PMC article.
-
Coverage of routine reporting on malaria parasitological testing in Kenya, 2015-2016.Glob Health Action. 2017;10(1):1413266. doi: 10.1080/16549716.2017.1413266. Glob Health Action. 2017. PMID: 29261450 Free PMC article.
References
-
- Breman J. The ears of the hippopotamus: manifestations, determinants, and estimates of the malaria burden. Am J Trop Med Hyg. 2001;64:1–11. - PubMed
-
- Agyepong IA, Kangeya-Kayonda J. Providing practical estimates of malaria burden for health planners in resource-poor countries. Am J Trop Med Hyg. 2004;71:162–7. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
