

Prediction of excess weight loss after laparoscopic Roux-en-Y gastric bypass: data from an artificial neural network
- PMID: 26017908
- PMCID: PMC4662927
- DOI: 10.1007/s00464-015-4225-7
Prediction of excess weight loss after laparoscopic Roux-en-Y gastric bypass: data from an artificial neural network
Abstract
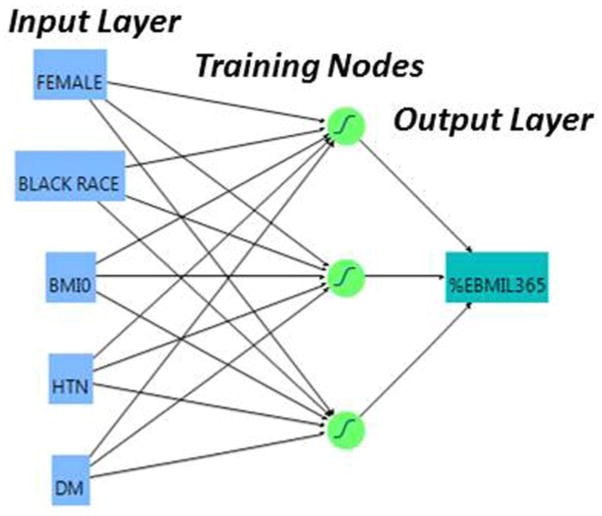
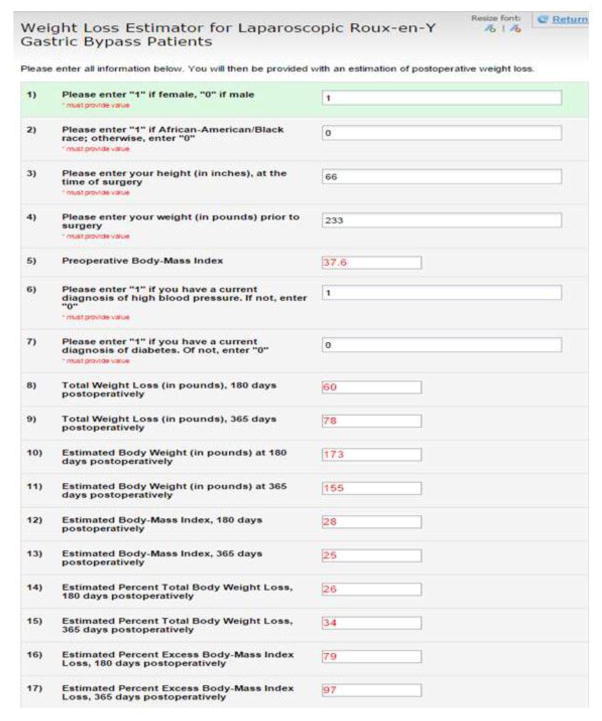
Introduction: Laparoscopic Roux-en-Y gastric bypass (LRYGB) has become the gold standard for surgical weight loss. The success of LRYGB may be measured by excess body mass index loss (%EBMIL) over 25 kg/m(2), which is partially determined by multiple patient factors. In this study, artificial neural network (ANN) modeling was used to derive a reasonable estimate of expected postoperative weight loss using only known preoperative patient variables. Additionally, ANN modeling allowed for the discriminant prediction of achievement of benchmark 50% EBMIL at 1 year postoperatively.
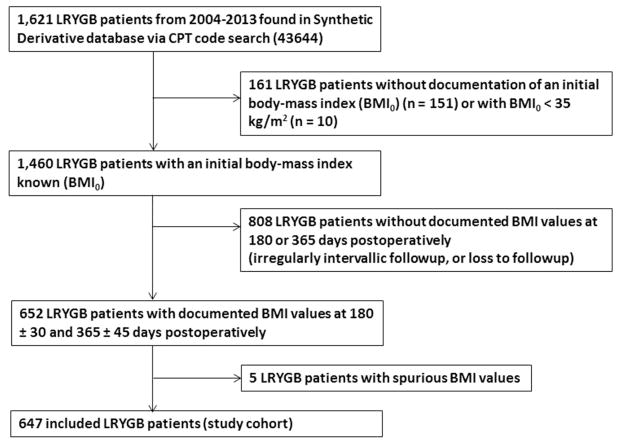
Methods: Six hundred and forty-seven LRYGB included patients were retrospectively reviewed for preoperative factors independently associated with EBMIL at 180 and 365 days postoperatively (EBMIL180 and EBMIL365, respectively). Previously validated factors were selectively analyzed, including age; race; gender; preoperative BMI (BMI0); hemoglobin; and diagnoses of hypertension (HTN), diabetes mellitus (DM), and depression or anxiety disorder. Variables significant upon multivariate analysis (P < .05) were modeled by "traditional" multiple linear regression and an ANN, to predict %EBMIL180 and %EBMIL365.
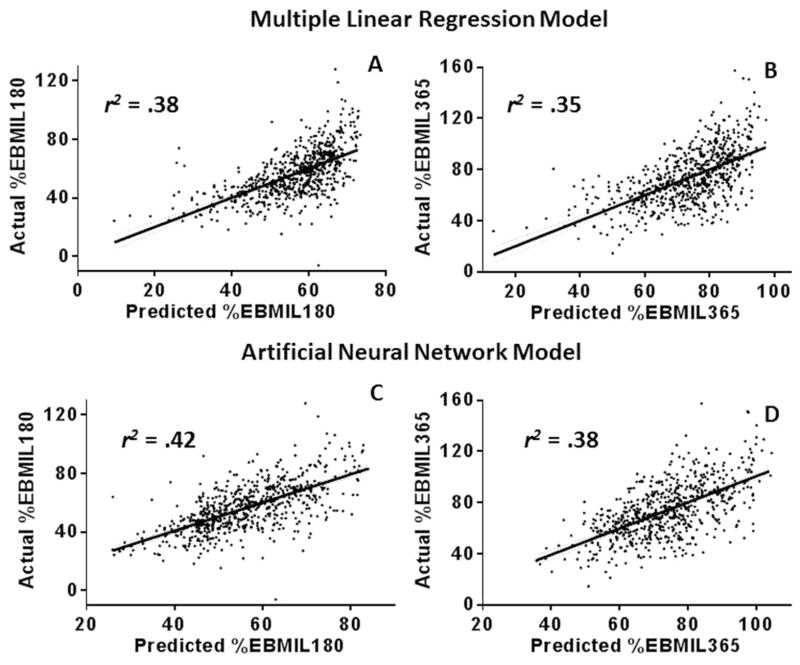
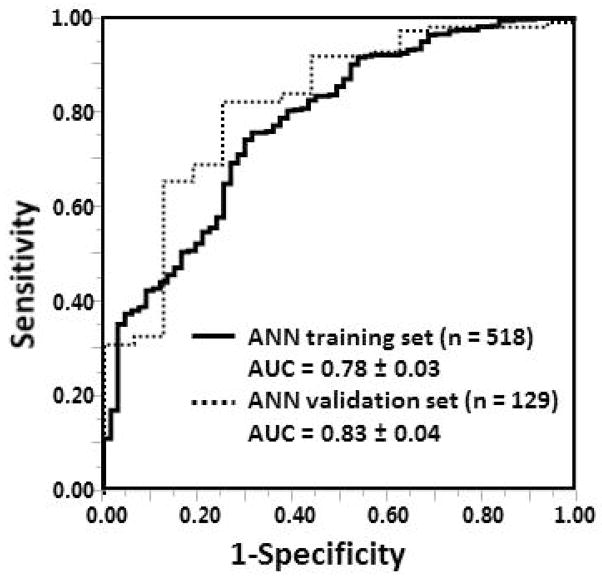
Results: The mean EBMIL180 and EBMIL365 were 56.4 ± 16.5 % and 73.5 ± 21.5%, corresponding to total body weight losses of 25.7 ± 5.9% and 33.6 ± 8.0%, respectively. Upon multivariate analysis, independent factors associated with EBMIL180 included black race (B = -6.3%, P < .001), BMI0 (B = -1.1%/unit BMI, P < .001), and DM (B = -3.2%, P < .004). For EBMIL365, independently associated factors were female gender (B = 6.4%, P < .001), black race (B = -6.7%, P < .001), BMI0 (B = -1.2%/unit BMI, P < .001), HTN (B = -3.7%, P = .03), and DM (B = -6.0%, P < .001). Pearson r(2) values for the multiple linear regression and ANN models were 0.38 (EBMIL180) and 0.35 (EBMIL365), and 0.42 (EBMIL180) and 0.38 (EBMIL365), respectively. ANN prediction of benchmark 50% EBMIL at 365 days generated an area under the curve of 0.78 ± 0.03 in the training set (n = 518) and 0.83 ± 0.04 (n = 129) in the validation set.
Conclusions: Available at https://redcap.vanderbilt.edu/surveys/?s=3HCR43AKXR, this or other ANN models may be used to provide an optimized estimate of postoperative EBMIL following LRYGB.
Keywords: Bariatric; Gastric bypass; Obesity; Outcomes.
Conflict of interest statement
Eric Wise, Kyle Hocking and Stephen Kavic have no conflict of interest to disclose.
Figures
Similar articles
-
Red cell distribution width is a novel biomarker that predicts excess body-mass index loss 1 year after laparoscopic Roux-en-Y gastric bypass.Surg Endosc. 2016 Oct;30(10):4607-12. doi: 10.1007/s00464-016-4798-9. Epub 2016 Feb 22. Surg Endosc. 2016. PMID: 26902617 Free PMC article.
-
Baseline Anthropometric and Metabolic Parameters Correlate with Weight Loss in Women 1-Year After Laparoscopic Roux-En-Y Gastric Bypass.Obes Surg. 2017 Nov;27(11):2940-2949. doi: 10.1007/s11695-017-2720-8. Obes Surg. 2017. PMID: 28550439 Clinical Trial.
-
Predictors of Inadequate Weight Loss After Laparoscopic Gastric Bypass for Morbid Obesity.Obes Surg. 2017 Jun;27(6):1446-1452. doi: 10.1007/s11695-016-2500-x. Obes Surg. 2017. PMID: 27943095
-
Long-term weight loss of distal gastric bypass is moderately superior compared to proximal gastric bypass in patients with a BMI of 37-44 Kg/m2.Langenbecks Arch Surg. 2024 May 21;409(1):162. doi: 10.1007/s00423-024-03348-2. Langenbecks Arch Surg. 2024. PMID: 38771517 Free PMC article.
-
Comparative analysis of weight loss and resolution of comorbidities between laparoscopic sleeve gastrectomy and Roux-en-Y gastric bypass: A systematic review and meta-analysis based on 18 studies.Int J Surg. 2020 Apr;76:101-110. doi: 10.1016/j.ijsu.2020.02.035. Epub 2020 Mar 6. Int J Surg. 2020. PMID: 32151750
Cited by
-
Weight Loss Prediction after Metabolic and Bariatric Surgery.J Obes Metab Syndr. 2023 Mar 30;32(1):46-54. doi: 10.7570/jomes23008. Epub 2023 Mar 22. J Obes Metab Syndr. 2023. PMID: 36945076 Free PMC article. Review.
-
A Matched Cohort Analysis of Stomach Intestinal Pylorus Saving (SIPS) Surgery Versus Biliopancreatic Diversion with Duodenal Switch with Two-Year Follow-up.Obes Surg. 2017 Feb;27(2):454-461. doi: 10.1007/s11695-016-2341-7. Obes Surg. 2017. PMID: 27568033
-
Current Applications of Artificial Intelligence in Bariatric Surgery.Obes Surg. 2022 Aug;32(8):2717-2733. doi: 10.1007/s11695-022-06100-1. Epub 2022 May 26. Obes Surg. 2022. PMID: 35616768 Free PMC article. Review.
-
A matched cohort analysis of single anastomosis loop duodenal switch versus Roux-en-Y gastric bypass with 18-month follow-up.Surg Endosc. 2016 Sep;30(9):3958-64. doi: 10.1007/s00464-015-4707-7. Epub 2015 Dec 22. Surg Endosc. 2016. PMID: 26694182
-
Red cell distribution width is a novel biomarker that predicts excess body-mass index loss 1 year after laparoscopic Roux-en-Y gastric bypass.Surg Endosc. 2016 Oct;30(10):4607-12. doi: 10.1007/s00464-016-4798-9. Epub 2016 Feb 22. Surg Endosc. 2016. PMID: 26902617 Free PMC article.
References
-
- Carter J, Elliott S, Kaplan J, Lin M, Posselt A, Rogers S. Predictors of hospital stay following laparoscopic gastric bypass: analysis of 9,593 patients from the National Surgical Quality Improvement Program. Surgery for obesity and related diseases : official journal of the American Society for Bariatric Surgery 2014 - PubMed
-
- Tadross JA, le Roux CW. The mechanisms of weight loss after bariatric surgery. International journal of obesity. 2009;33(Suppl 1):S28–32. - PubMed
-
- Levine MS, Carucci LR. Imaging of bariatric surgery: normal anatomy and postoperative complications. Radiology. 2014;270:327–341. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
