

Recommendations for standardized pathological characterization of residual disease for neoadjuvant clinical trials of breast cancer by the BIG-NABCG collaboration
- PMID: 26019189
- PMCID: PMC4804123
- DOI: 10.1093/annonc/mdv161
Recommendations for standardized pathological characterization of residual disease for neoadjuvant clinical trials of breast cancer by the BIG-NABCG collaboration
Abstract
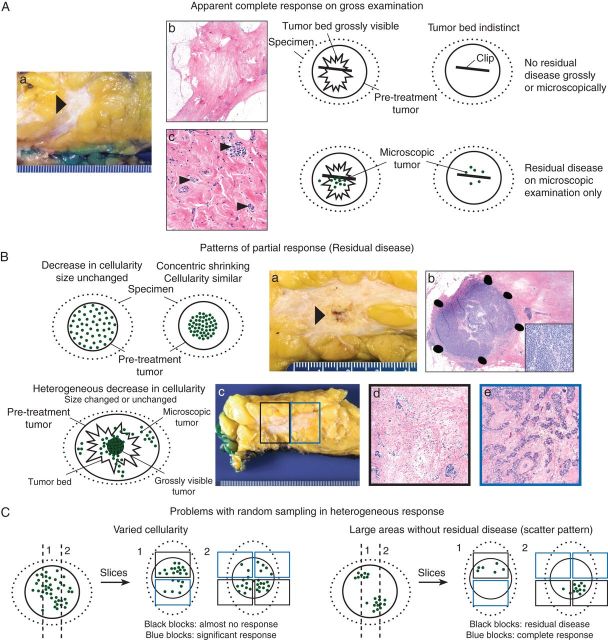
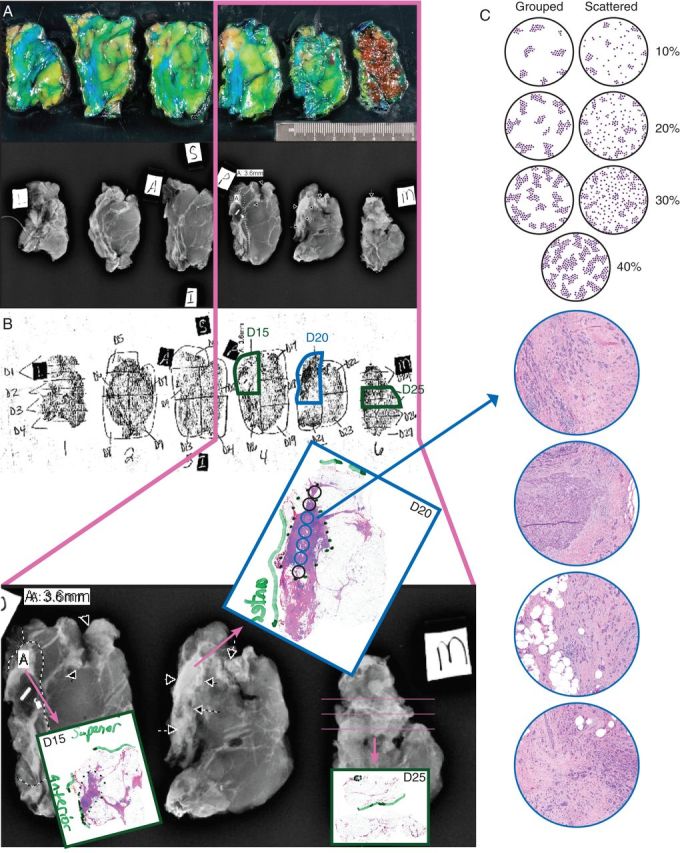
Neoadjuvant systemic therapy (NAST) provides the unique opportunity to assess response to treatment after months rather than years of follow-up. However, significant variability exists in methods of pathologic assessment of response to NAST, and thus its interpretation for subsequent clinical decisions. Our international multidisciplinary working group was convened by the Breast International Group-North American Breast Cancer Group (BIG-NABCG) collaboration and tasked to recommend practical methods for standardized evaluation of the post-NAST surgical breast cancer specimen for clinical trials that promote accurate and reliable designation of pathologic complete response (pCR) and meaningful characterization of residual disease. Recommendations include multidisciplinary communication; clinical marking of the tumor site (clips); and radiologic, photographic, or pictorial imaging of the sliced specimen, to map the tissue sections and reconcile macroscopic and microscopic findings. The information required to define pCR (ypT0/is ypN0 or ypT0 yp N0), residual ypT and ypN stage using the current AJCC/UICC system, and the Residual Cancer Burden system were recommended for quantification of residual disease in clinical trials.
Keywords: breast cancer; neoadjuvant systemic therapy; pathologic assessment; pathologic complete response; residual disease; response evaluation.
© The Author 2015. Published by Oxford University Press on behalf of the European Society for Medical Oncology. All rights reserved. For permissions, please email: journals.permissions@oup.com.
Figures
References
-
- Cortazar P, Zhang L, Untch M et al. . Pathological complete response and long-term clinical benefit in breast cancer: the CTNeoBC pooled analysis. Lancet 2014; 384: 164–172. - PubMed
-
- von Minckwitz G, Untch M, Blohmer JU et al. . Definition and impact of pathologic complete response on prognosis after neoadjuvant chemotherapy in various intrinsic breast cancer subtypes. J Clin Oncol 2012; 30: 1796–1804. - PubMed
-
- Esserman LJ, Woodcock J. Accelerating identification and regulatory approval of investigational cancer drugs. JAMA 2011; 306: 2608–2609. - PubMed
-
- U.S. Food and Drug Administration. Guidance for industry: pathological complete response in neoadjuvant treatment of high-risk early-stage breast cancer: use as an endpoint to support accelerated approval. 2014. http://www.fda.gov/downloads/Drugs/GuidanceComplianceRegulatoryInformati... (30 October 2014, date last accessed).
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
