

Abnormal contrast responses in the extrastriate cortex of blindsight patients
- PMID: 26019336
- PMCID: PMC4444542
- DOI: 10.1523/JNEUROSCI.3075-14.2015
Abnormal contrast responses in the extrastriate cortex of blindsight patients
Abstract
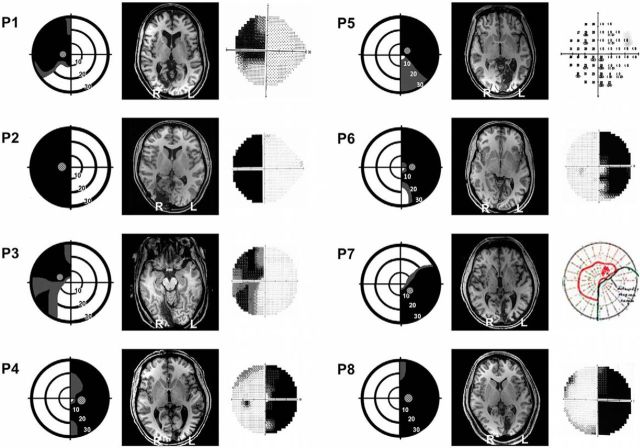
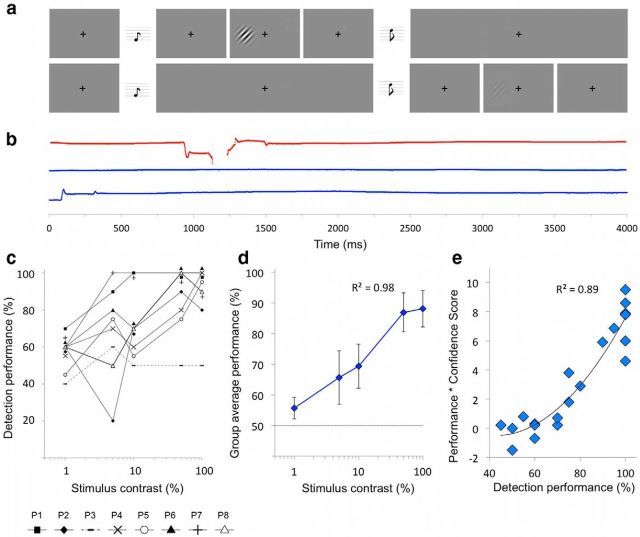
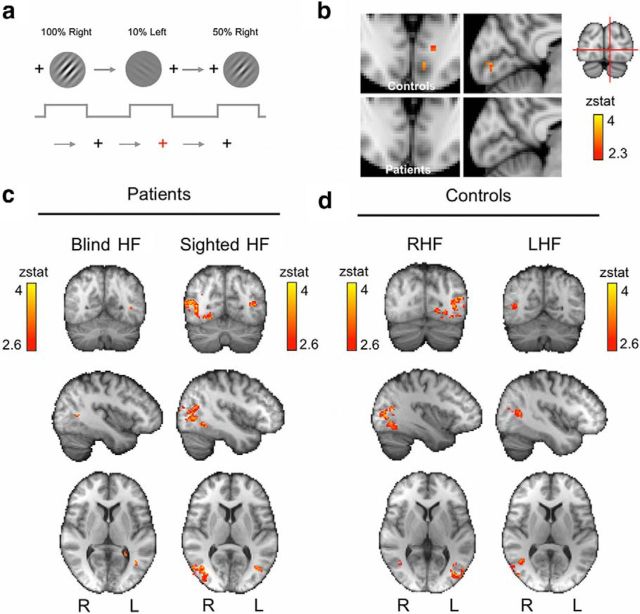
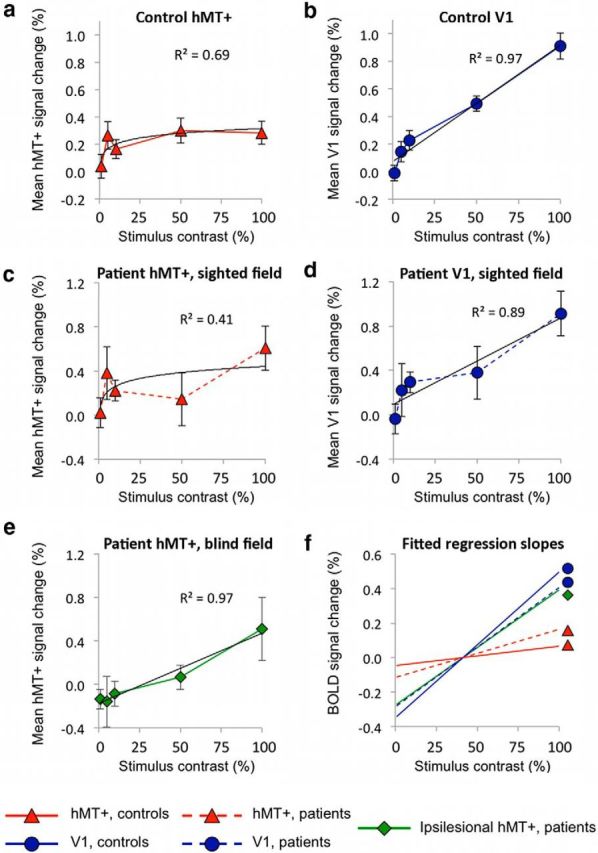
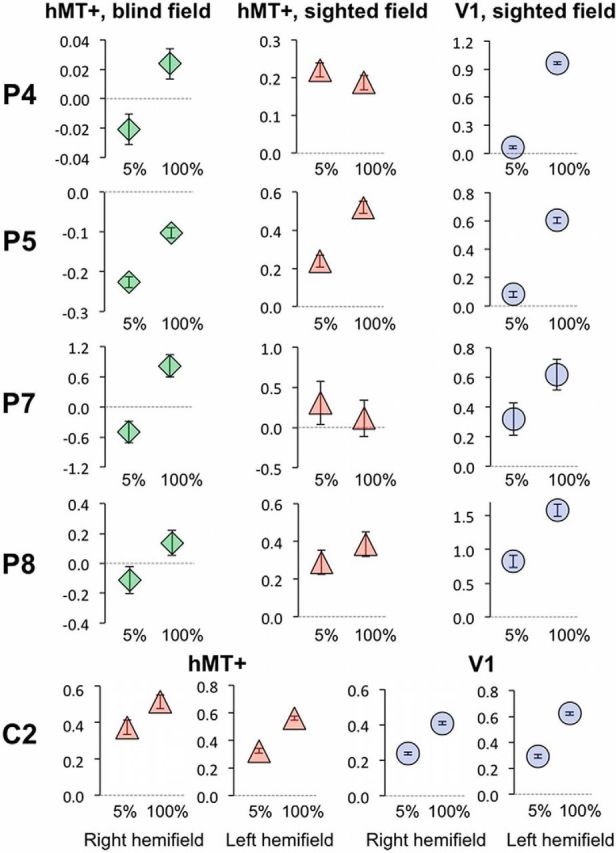
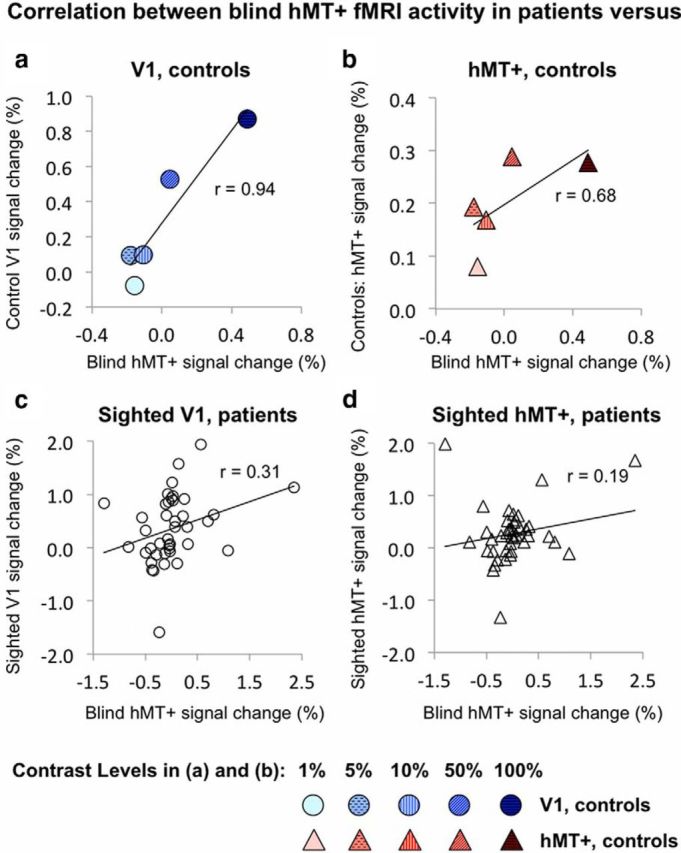
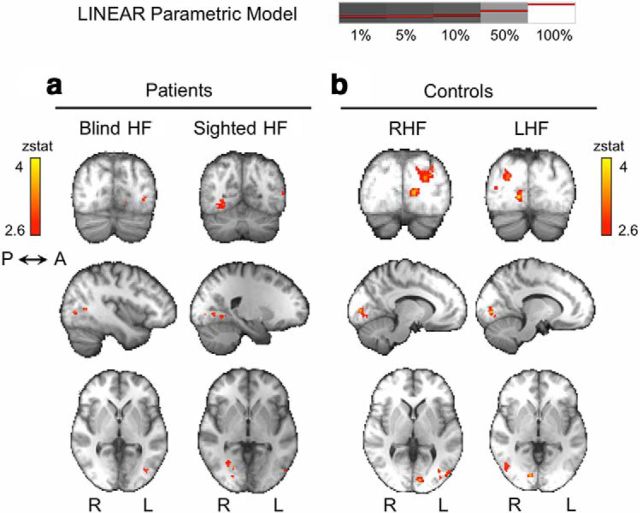
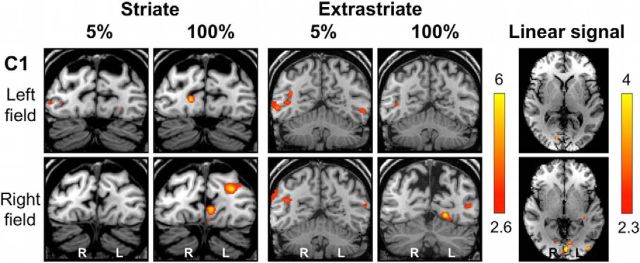
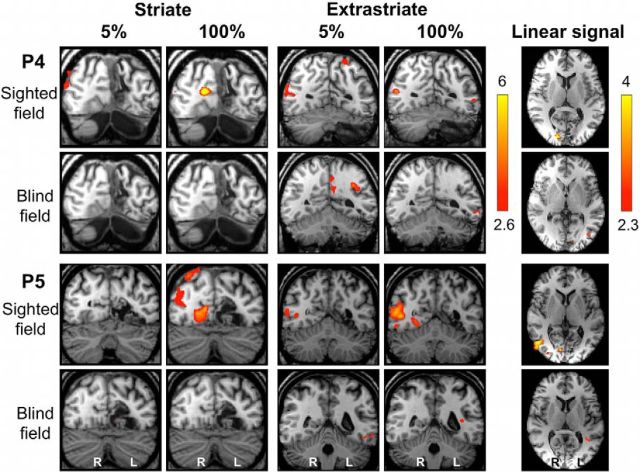
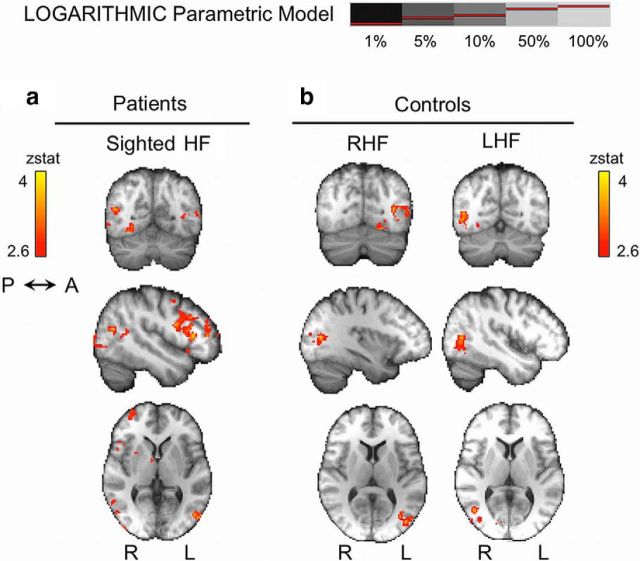
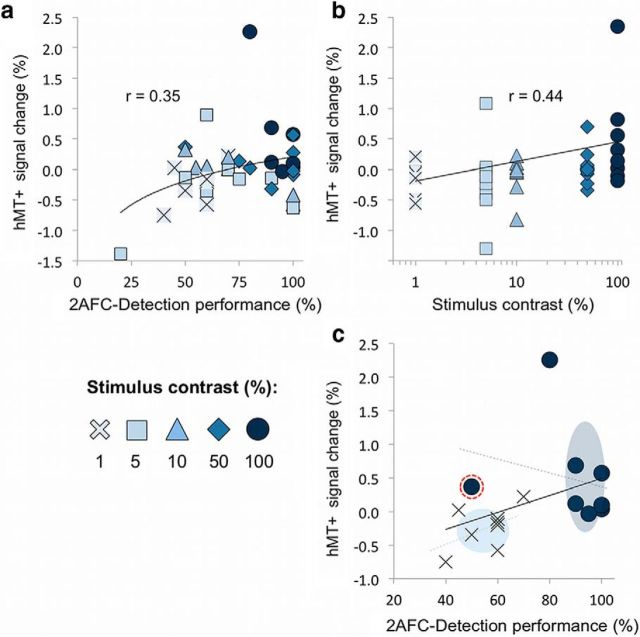
When the human primary visual cortex (V1) is damaged, the dominant geniculo-striate pathway can no longer convey visual information to the occipital cortex. However, many patients with such damage retain some residual visual function that must rely on an alternative pathway directly to extrastriate occipital regions. This residual vision is most robust for moving stimuli, suggesting a role for motion area hMT+. However, residual vision also requires high-contrast stimuli, which is inconsistent with hMT+ sensitivity to contrast in which even low-contrast levels elicit near-maximal neural activation. We sought to investigate this discrepancy by measuring behavioral and neural responses to increasing contrast in patients with V1 damage. Eight patients underwent behavioral testing and functional magnetic resonance imaging to record contrast sensitivity in hMT+ of their damaged hemisphere, using Gabor stimuli with a spatial frequency of 1 cycle/°. The responses from hMT+ of the blind hemisphere were compared with hMT+ and V1 responses in the sighted hemisphere of patients and a group of age-matched controls. Unlike hMT+, neural responses in V1 tend to increase linearly with increasing contrast, likely reflecting a dominant parvocellular channel input. Across all patients, the responses in hMT+ of the blind hemisphere no longer showed early saturation but increased linearly with contrast. Given the spatiotemporal parameters used in this study and the known direct subcortical projections from the koniocellular layers of the lateral geniculate nucleus to hMT+, we propose that this altered contrast sensitivity in hMT+ could be consistent with input from the koniocellular pathway.
Keywords: V1; blindsight; contrast; fMRI; hMT+; hemianopia.
Copyright © 2015 the authors 0270-6474/15/358201-13$15.00/0.
Figures
References
-
- Albrecht DG, Hamilton DB. Striate cortex of monkey and cat: contrast response function. J Neurophysiol. 1982;48:217–237. - PubMed
-
- Andersson JLR, Jenkinson M, Smith SM. Functional MRI of the Brain technical report. Oxford, UK: TR07JA1; 2007. Non-linear optimisation.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources