

Implementation of Intraoperative Neurophysiological Monitoring during Endovascular Procedures in the Central Nervous System
- PMID: 26019712
- PMCID: PMC4439781
- DOI: 10.1159/000371453
Implementation of Intraoperative Neurophysiological Monitoring during Endovascular Procedures in the Central Nervous System
Abstract
Background and objective: Intraoperative monitoring (IOM) has been used in different surgical disciplines since the 1980s. Nonetheless, regular routine use of IOM in interventional neuroradiology units has only been reported in a few centers. The aim of this study is to report our experience, 1 year after deciding to implement standardized IOM during endovascular treatment of vascular abnormalities of the central nervous system.
Methods: Basic recordings included somatosensory-evoked potentials (SEPs) and motor-evoked potentials (MEPs). Corticobulbar motor-evoked potentials and flash-visual-evoked potentials were also recorded depending on the topography of the lesion. Intra-arterial provocative tests (PTs) with amobarbital and lidocaine were also performed. All patients except 1 were under total intravenous anesthesia. Clinical outcome was assessed prospectively and correlated with IOM events.
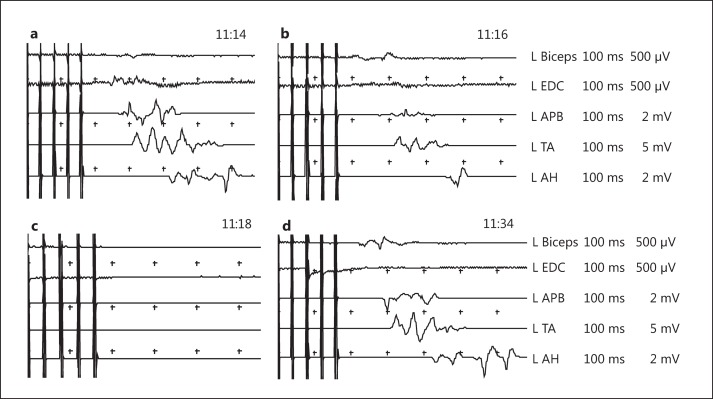
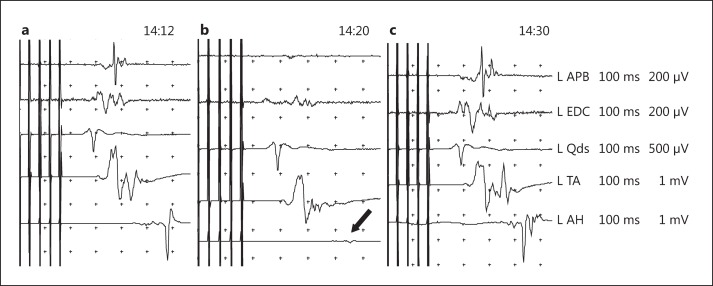
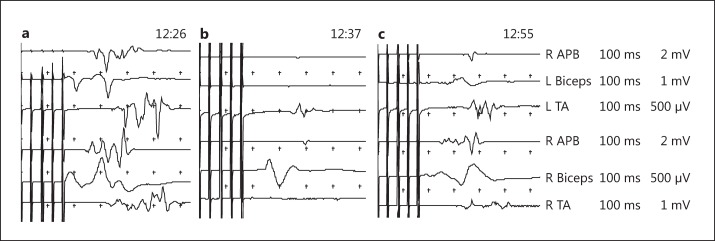
Results: Twelve patients and 15 procedures were monitored during the inclusion period. Significant IOM events were detected during 3 of the 15 procedures (20%). We observed temporary MEP changes in 2 cases which resolved after interruption of the embolization or application of corrective measures, leaving no postoperative neurological deficits. In 1 case, persistent SEP and MEP deterioration was detected secondary to a frontal hematoma, resulting in mild sensory-motor deficit in the right upper extremity after the procedure. Overall, 12 PTs (4 spinal cord and 8 brain abnormalities) were performed using lidocaine and sodium amytal injections. One positive result occurred after the injection of lidocaine. No false negatives were detected.
Conclusions: IOM may provide continuous real-time data about the functional status of eloquent areas and pathways of the central nervous system in patients under general anesthesia. It therefore allows us to detect early neurological damage in time to perform specific actions that may prevent irreversible neurological deficits.
Keywords: Central nervous system, vascular pathology; Endovascular treatment; Evoked potentials; Intraoperative neurophysiological monitoring; Provocative tests.
Figures
Similar articles
-
Neurophysiologic monitoring and pharmacologic provocative testing for embolization of spinal cord arteriovenous malformations.AJNR Am J Neuroradiol. 2004 Aug;25(7):1131-8. AJNR Am J Neuroradiol. 2004. PMID: 15313696 Free PMC article.
-
Neuroprotective role of neurophysiological monitoring during endovascular procedures in the brain and spinal cord.Neurophysiol Clin. 2007 Dec;37(6):415-21. doi: 10.1016/j.neucli.2007.10.004. Epub 2007 Nov 9. Neurophysiol Clin. 2007. PMID: 18083497
-
Neuroprotective role of neurophysiological monitoring during endovascular procedures in the spinal cord.Ann N Y Acad Sci. 2001 Jun;939:126-36. doi: 10.1111/j.1749-6632.2001.tb03619.x. Ann N Y Acad Sci. 2001. PMID: 11462764
-
Intraoperative neurophysiological monitoring in pediatric neurosurgery: why, when, how?Childs Nerv Syst. 2002 Jul;18(6-7):264-87. doi: 10.1007/s00381-002-0582-3. Epub 2002 Jun 13. Childs Nerv Syst. 2002. PMID: 12172930 Review.
-
Intraoperative Neurophysiological Monitoring : A Review of Techniques Used for Brain Tumor Surgery in Children.J Korean Neurosurg Soc. 2018 May;61(3):363-375. doi: 10.3340/jkns.2018.0078. Epub 2018 May 1. J Korean Neurosurg Soc. 2018. PMID: 29742889 Free PMC article. Review.
Cited by
-
Intraoperative Neuromonitoring for Cerebral Arteriovenous Malformation Embolization: A Propensity-Score Matched Retrospective Database Study.Cureus. 2021 Jan 27;13(1):e12946. doi: 10.7759/cureus.12946. Cureus. 2021. PMID: 33654622 Free PMC article.
-
Motor Evoked Potential Warning Criteria in Supratentorial Surgery: A Scoping Review.Cancers (Basel). 2021 Jun 4;13(11):2803. doi: 10.3390/cancers13112803. Cancers (Basel). 2021. PMID: 34199853 Free PMC article.
-
Comparing the effect between continuous infusion and intermittent bolus of rocuronium for intraoperative neurophysiologic monitoring of neurointervention under general anesthesia.Medicine (Baltimore). 2018 Dec;97(51):e13816. doi: 10.1097/MD.0000000000013816. Medicine (Baltimore). 2018. PMID: 30572545 Free PMC article. Clinical Trial.
-
Intraoperative motor-evoked potential monitoring during coil embolization for anterior choroidal artery aneurysms.Neuroradiology. 2022 Jun;64(6):1221-1229. doi: 10.1007/s00234-021-02847-z. Epub 2021 Nov 17. Neuroradiology. 2022. PMID: 34791541
References
-
- Niimi Y, Deletis V, Berenstein A. Neurophysiological monitoring during spinal endovascular procedures; in Nuwer MR (ed): Intraoperative Monitoring of Neural Function – Handbook of Clinical Neurophysiology. Amsterdam, Elsevier. 2008:651.
-
- Berenstein A, Young W, Ransohoff J, Benjamin V, Merkin H. Somatosensory evoked potentials during spinal angiography and therapeutic transvascular embolization. J Neurosurg. 1984;60:777–785. - PubMed
-
- Hacke W. Evoked potentials monitoring in interventional neuroradiology; in Desmedt JE (ed): Neuromonitoring in Surgery. Amsterdam, Elsevier. 1989:331–342.
-
- Ginsburg HH, Shetter AG, Raudzens PA. Postoperative paraplegia with preserved intraoperative somatosensory evoked potentials. Case report. J Neurosurg. 1985;63:296–300. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
