

Management of hyperphosphataemia in chronic kidney disease-challenges and solutions
- PMID: 26019840
- PMCID: PMC4432434
- DOI: 10.1093/ckj/sfs173
Management of hyperphosphataemia in chronic kidney disease-challenges and solutions
Abstract
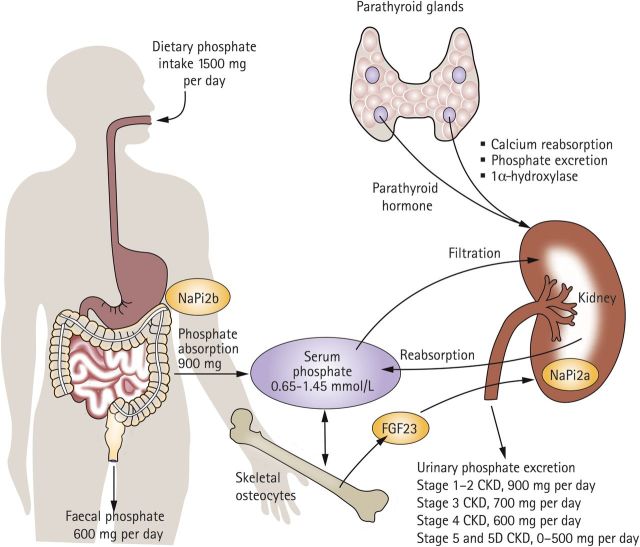
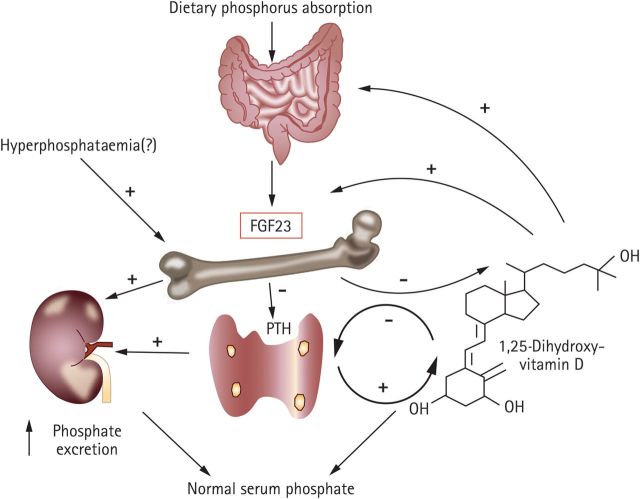
Hyperphosphataemia is a clinical consequence of the advanced stages of chronic kidney disease (CKD). Considerable evidence points to a role of hyperphosphataemia in the pathogenesis of CKD-associated cardiovascular (CV) complications, including vascular calcification, and with increased all-cause and CV mortality. These observations place management of hyperphosphataemia at the centre of CKD treatment. Although our increased understanding of the physiological role of FGF-23 may provide a long-term alternative biomarker of phosphate load and underlying disease progression, regular determination of serum phosphate is currently the most frequently used parameter to evaluate phosphate load in clinical practice. This review considers the challenges physicians and patients face in trying to control hyperphosphataemia. Amongst these are the limitations of dietary phosphate restriction, giving rise to the need for phosphate binder therapy to maintain serum phosphate control. Once the decision to use phosphate binders has been made, considerations include the relative efficacy, different potential side effects and pill burden associated with various phosphate binders. Although a number of phosphate binders are available, adherence poses a major obstacle to effective treatment. This emphasizes that further improvements to phosphate binder therapy can be made. Evaluation of novel agents and their potential role in the clinic should continue.
Keywords: chronic kidney disease; hyperphosphataemia; phosphate binder.
Figures
References
-
- Zhang QL, Rothenbacher D. Prevalence of chronic kidney disease in population-based studies: systematic review. BMC Public Health. 2008;8:117. doi:10.1186/1471-2458-8-117. - DOI - PMC - PubMed
-
- Couser WG, Remuzzi G, Mendis S, et al. The contribution of chronic kidney disease to the global burden of major noncommunicable diseases. Kidney Int. 2011;80:1258–1270. doi:10.1038/ki.2011.368. - DOI - PubMed
-
- Kidney Disease: Improving Global Outcomes. KDIGO clinical practice guideline for the diagnosis, evaluation, prevention, and treatment of chronic kidney disease–mineral and bone disorder (CKD–MBD) Kidney Int Suppl. 2009;76:S1–S130. - PubMed
-
- Kasiske BL, Zeier MG, Chapman JR, et al. KDIGO clinical practice guideline for the care of kidney transplant recipients: a summary. Kidney Int. 2010;77:299–311. doi:10.1038/ki.2009.377. - DOI - PubMed
-
- Giachelli CM. The emerging role of phosphate in vascular calcification. Kidney Int. 2009;75:890–897. doi:10.1038/ki.2008.644. - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
