

Insulin therapy and dietary adjustments to normalize glycemia and prevent nocturnal hypoglycemia after evening exercise in type 1 diabetes: a randomized controlled trial
- PMID: 26019878
- PMCID: PMC4442134
- DOI: 10.1136/bmjdrc-2015-000085
Insulin therapy and dietary adjustments to normalize glycemia and prevent nocturnal hypoglycemia after evening exercise in type 1 diabetes: a randomized controlled trial
Abstract
Introduction: Evening-time exercise is a frequent cause of severe hypoglycemia in type 1 diabetes, fear of which deters participation in regular exercise. Recommendations for normalizing glycemia around exercise consist of prandial adjustments to bolus insulin therapy and food composition, but this carries only short-lasting protection from hypoglycemia. Therefore, this study aimed to examine the impact of a combined basal-bolus insulin dose reduction and carbohydrate feeding strategy on glycemia and metabolic parameters following evening exercise in type 1 diabetes.
Methods: Ten male participants (glycated hemoglobin: 52.4±2.2 mmol/mol), treated with multiple daily injections, completed two randomized study-days, whereby administration of total daily basal insulin dose was unchanged (100%), or reduced by 20% (80%). Participants attended the laboratory at ∼08:00 h for a fasted blood sample, before returning in the evening. On arrival (∼17:00 h), participants consumed a carbohydrate meal and administered a 75% reduced rapid-acting insulin dose and 60 min later performed 45 min of treadmill running. At 60 min postexercise, participants consumed a low glycemic index (LGI) meal and administered a 50% reduced rapid-acting insulin dose, before returning home. At ∼23:00 h, participants consumed a LGI bedtime snack and returned to the laboratory the following morning (∼08:00 h) for a fasted blood sample. Venous blood samples were analyzed for glucose, glucoregulatory hormones, non-esterified fatty acids, β-hydroxybutyrate, interleukin 6, and tumor necrosis factor α. Interstitial glucose was monitored for 24 h pre-exercise and postexercise.
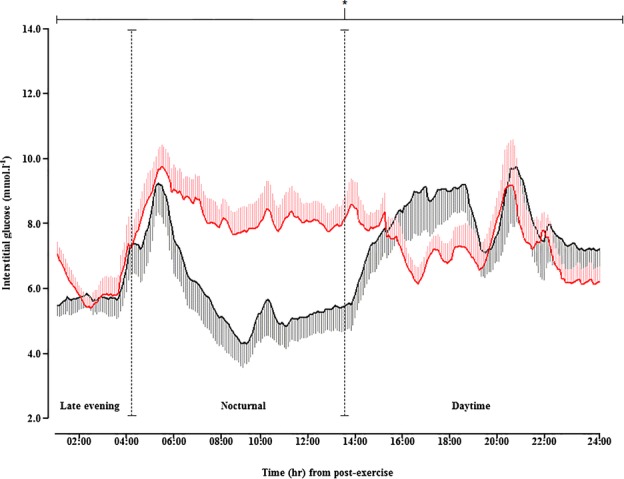
Results: Glycemia was similar until 6 h postexercise, with no hypoglycemic episodes. Beyond 6 h glucose levels fell during 100%, and nine participants experienced nocturnal hypoglycemia. Conversely, all participants during 80% were protected from nocturnal hypoglycemia, and remained protected for 24 h postexercise. All metabolic parameters were similar.
Conclusions: Reducing basal insulin dose with reduced prandial bolus insulin and LGI carbohydrate feeding provides protection from hypoglycemia during and for 24 h following evening exercise. This strategy is not associated with hyperglycemia, or adverse metabolic disturbances.
Clinical trials number: NCT02204839, ClinicalTrials.gov.
Keywords: Exercise; Hypoglycemia; Insulin; Type 1.
Figures


References
-
- American Diabetes Association. Diagnosis and classification of diabetes mellitus. Diabetes Care 2011;27:S5–S10. - PubMed
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical