

Observer variability in the assessment of CT coronary angiography and coronary artery calcium score: substudy of the Scottish COmputed Tomography of the HEART (SCOT-HEART) trial
- PMID: 26019881
- PMCID: PMC4442169
- DOI: 10.1136/openhrt-2014-000234
Observer variability in the assessment of CT coronary angiography and coronary artery calcium score: substudy of the Scottish COmputed Tomography of the HEART (SCOT-HEART) trial
Abstract
Introduction: Observer variability can influence the assessment of CT coronary angiography (CTCA) and the subsequent diagnosis of angina pectoris due to coronary heart disease.
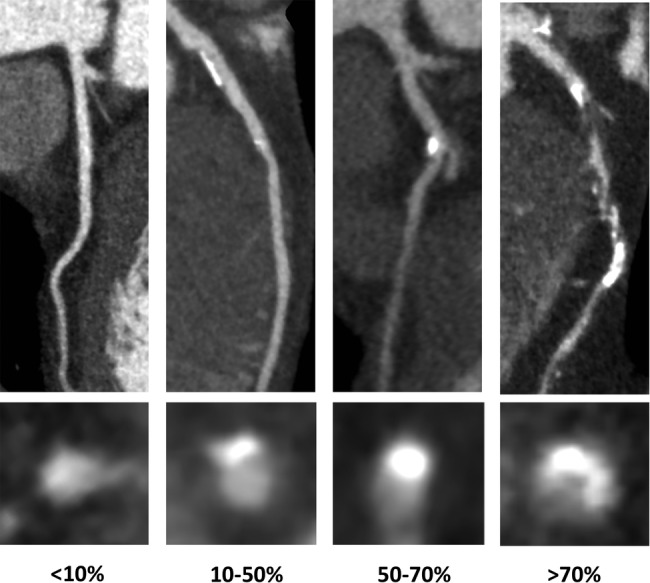
Methods: We assessed 210 CTCAs from the Scottish COmputed Tomography of the HEART (SCOT-HEART) trial for intraobserver and interobserver variability. Calcium score, coronary angiography and image quality were evaluated. Coronary artery disease was defined as none (<10%), mild (10-49%), moderate (50-70%) and severe (>70%) luminal stenosis and classified as no (<10%), non-obstructive (10-70%) or obstructive (>70%) coronary artery disease. Post-CTCA diagnosis of angina pectoris due to coronary heart disease was classified as yes, probable, unlikely or no.
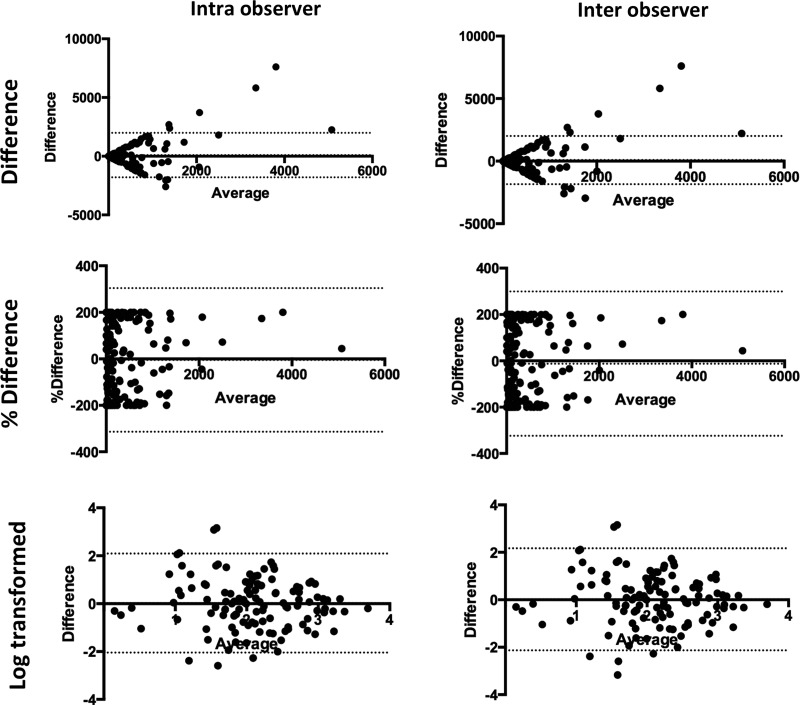
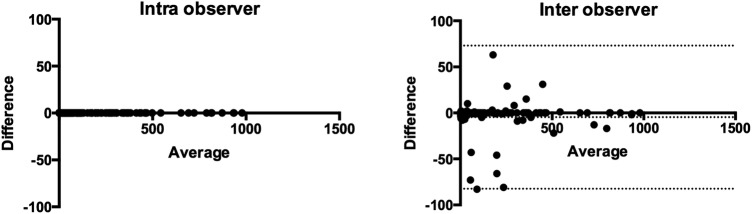
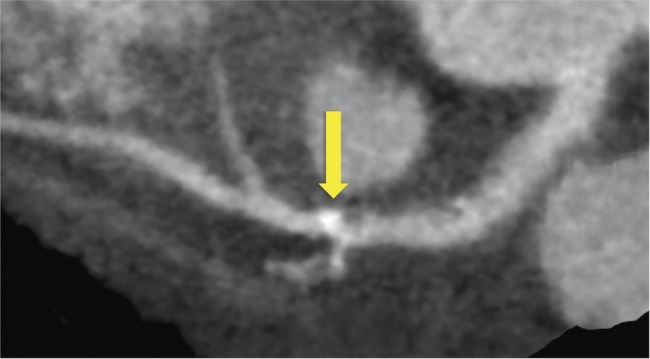
Results: Patients had a mean body mass index of 29 (28, 30) kg/m(2), heart rate of 58 (57, 60)/min and 62% were men. Intraobserver and interobserver agreements for the presence or absence of coronary artery disease were excellent (95% agreement, κ 0.884 (0.817 to 0.951) and good (91%, 0.791 (0.703 to 0.879)). Intraobserver and interobserver agreement for the presence or absence of angina pectoris due to coronary heart disease were excellent (93%, 0.842 (0.918 to 0.755) and good (86%, 0.701 (0.799 to 0.603)), respectively. Observer variability of calcium score was excellent for calcium scores below 1000. More segments were categorised as uninterpretable with 64-multidetector compared to 320-multidetector CTCA (10.1% vs 2.6%, p<0.001) but there was no difference in observer variability.
Conclusions: Multicentre multidetector CTCA has excellent agreement in patients under investigation for suspected angina due to coronary heart disease.
Trial registration number: NCT01149590.
Keywords: CHEST PAIN CLINIC < CORONARY ARTERY DISEASE; CORONARY ARTERY DISEASE; CT SCANNING < IMAGING AND DIAGNOSTICS; IMAGING AND DIAGNOSTICS.
Figures
References
-
- Newby DE, Williams MC, Flapan AD et al. . Role of multidetector computed tomography in the diagnosis and management of patients attending the rapid access chest pain clinic, The Scottish computed tomography of the heart (SCOT-HEART) trial: study protocol for randomized controlled trial. Trials 2012;13:184 10.1186/1745-6215-13-184 - DOI - PMC - PubMed
Publication types
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical